by Nithesh Ravindran | Mar 15, 2023
Case courtesy : Dr.Cicy Kuncherian Welcare Hospital
Age: 56Yrs
Sex: Female
Complaints: Right iliac fossa pain.
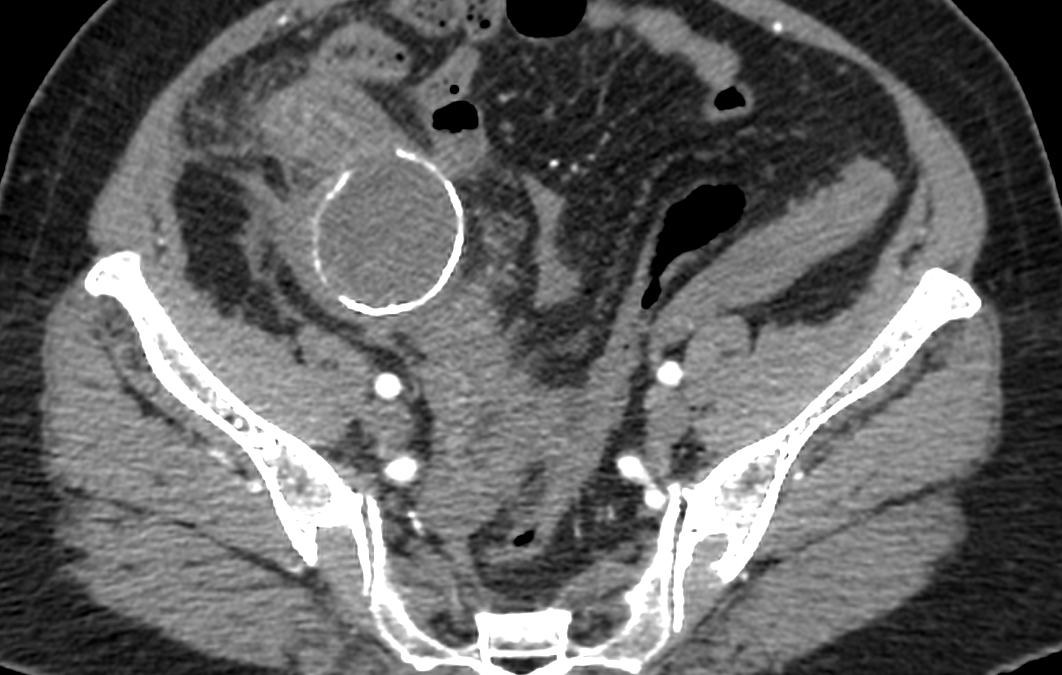
Case study: Tubular cystic mass lesion with peripheral enhancing walls measuring approximately 5.2 x4.3 x5.6 cm (TR XAP x CC) is seen in the right iliac fossa showing thick curvilinear mural calcification and central fluid density. No intraluminal air pockets noted.
The lesion is closely adherent towards the adjacent bowel loops causing bowel wall thickening of terminal ileum and cecum and adjacent fat stranding . Appendix not separately visualized from the mass lesion. Few prominent mesenteric lymph nodes are noted in right iliac fossa and paraumbilical region.
Small wall defect noted in the inferior aspect of the lesion with tubular extension measuring 14 x12mm extending into the right adnexa . Right ovary not separately
Images:



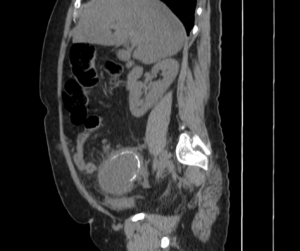

Conclusion : Tubular cystic mass lesion with curvilinear mural calcification in right iliac fossa with adjacent bowel wall thickening and fat stranding -features are in favor of Appendiceal Mucocele with contained perforation. Suggested lab correlation.
by Nithesh Ravindran | Mar 15, 2023
Case courtesy : Dr.Cicy Kuncherian,Welcare Hospital.
Age: 27 Yrs
Sex: Male
Complaints: Swelling frontal region.
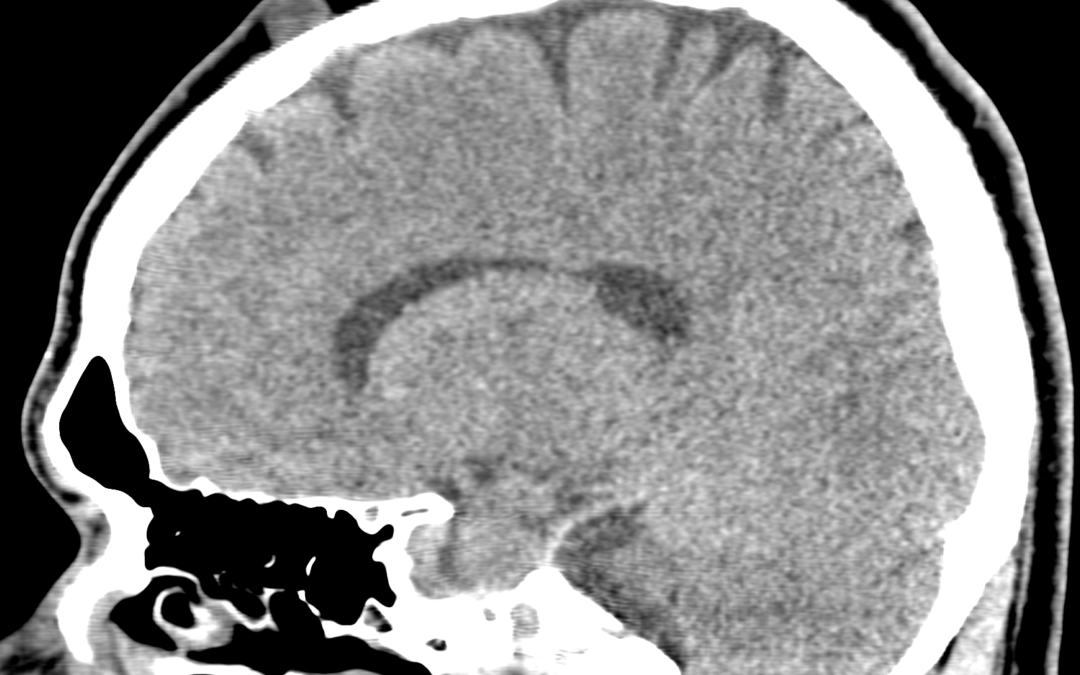
Case study: A well defined soft tissue density lesion (~ +13HU) measuring ~13 x 11 mm noted in the frontal region involving subgaleal layer. No evidence of intracranial invasion / bone erosion.
Images:
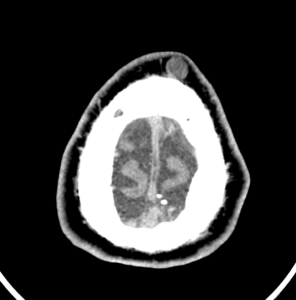
Conclusion :A well defined soft tissue lesion involving the mid frontal region causing superficial skin asymmetry as described – Imaging features in favour of dermoid cyst. Possible DD: Sebaceous cyst.

by Nithesh Ravindran | Dec 5, 2022
Case Courtesy : Dr Sajith Selvaganesan MD FSCCT FSCMR,Sunrise Hospital
Age: 25Yrs
Sex: Male
Complaints: Lower back pain.
Case study:
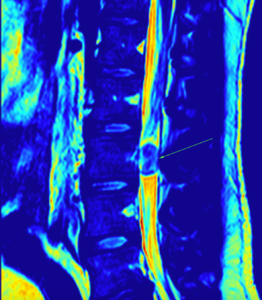
Loss of normal lumbar lordosis.
Relatively well defined, mildly heterogeneous, round to oval, iso to hyperintense intramedullary lesion measuring 11 x 10 x 17 mm (TR x AP x CC) noted the level of L3 vertebra
Images:


Conclusion
Relatively well defined, mildly heterogeneous, round to oval, iso to hyperintense intramedullary lesion measuring 11 x 10 x 17 mm (TR x AP x CC) noted the level of L3 vertebra – Likely myxopapillary ependymoma. Differential includes paraganglioma. Suggested HPE evaluation.
by Nithesh Ravindran | Dec 4, 2022
Case courtesy : Dr Sajith Selvaganesan MD FSCCT FSCMR, Sunrise Hospital
Age: 68 Yrs
Sex: Female
Case study:
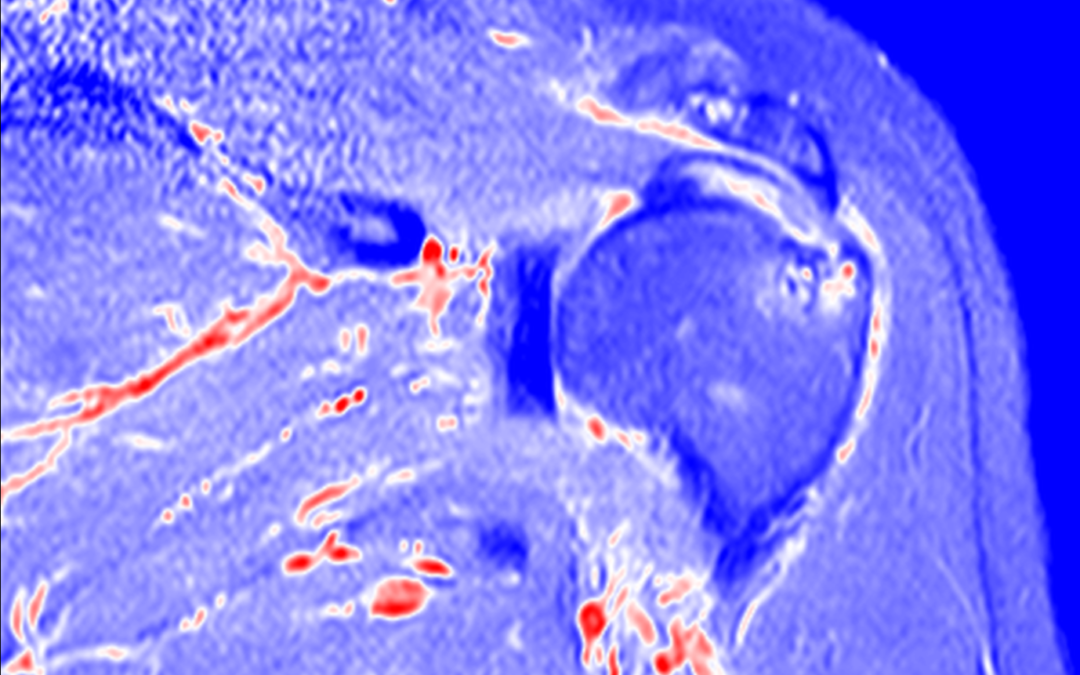
High grade partial tear of subscapularis tendon with no retraction of muscle.
Altered intra-substance signal intensity noted in the supraspinatus tendon reaching up to the articular surface.
Altered signal intensity noted in the posterolateral aspect of humeral head.
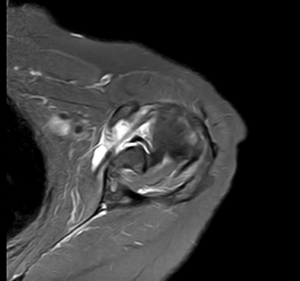
Type V superior labral anterior posterior tear noted with minimal fluid along the interface.
Type II acromion seen.
Minimal joint effusion with subcoracoid bursal fluid.
Images:
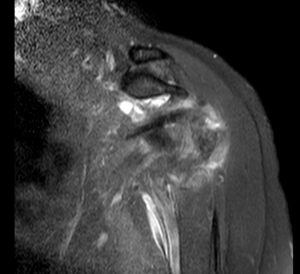
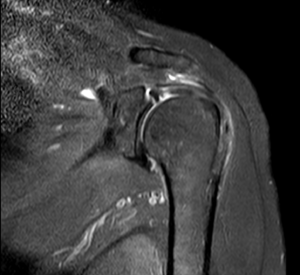
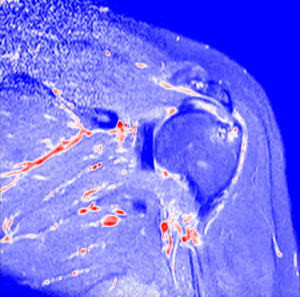
Conclusion :
High grade partial tear of subscapularis tendon.
Partial tear of supraspinatus tendon.
Type V superior labral anterior posterior tear.
Altered signal intensity in the posterolateral aspect of humeral head – Likely hillsach’s lesion.
Minimal joint effusion with subcoracoid bursal fluid.
Acromioclavicular joint athropathy changes.
by Nithesh Ravindran | Aug 28, 2022
Age: 28yr
Sex: Male
Complaints: Progressive walking difficulty.
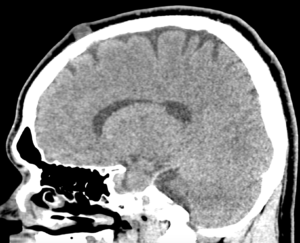
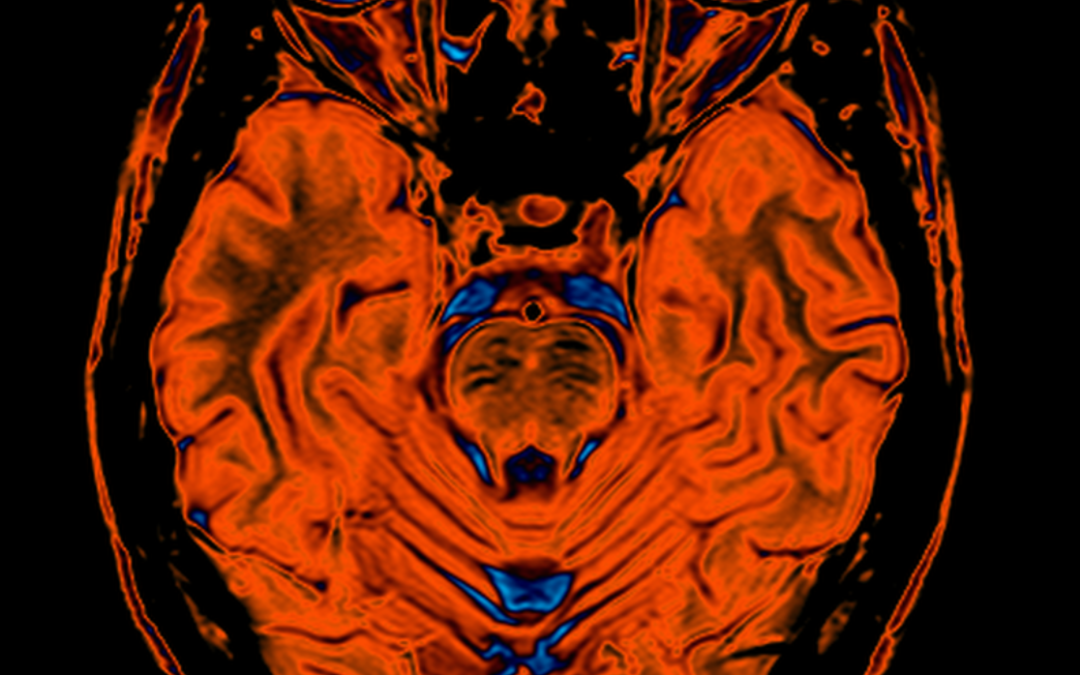
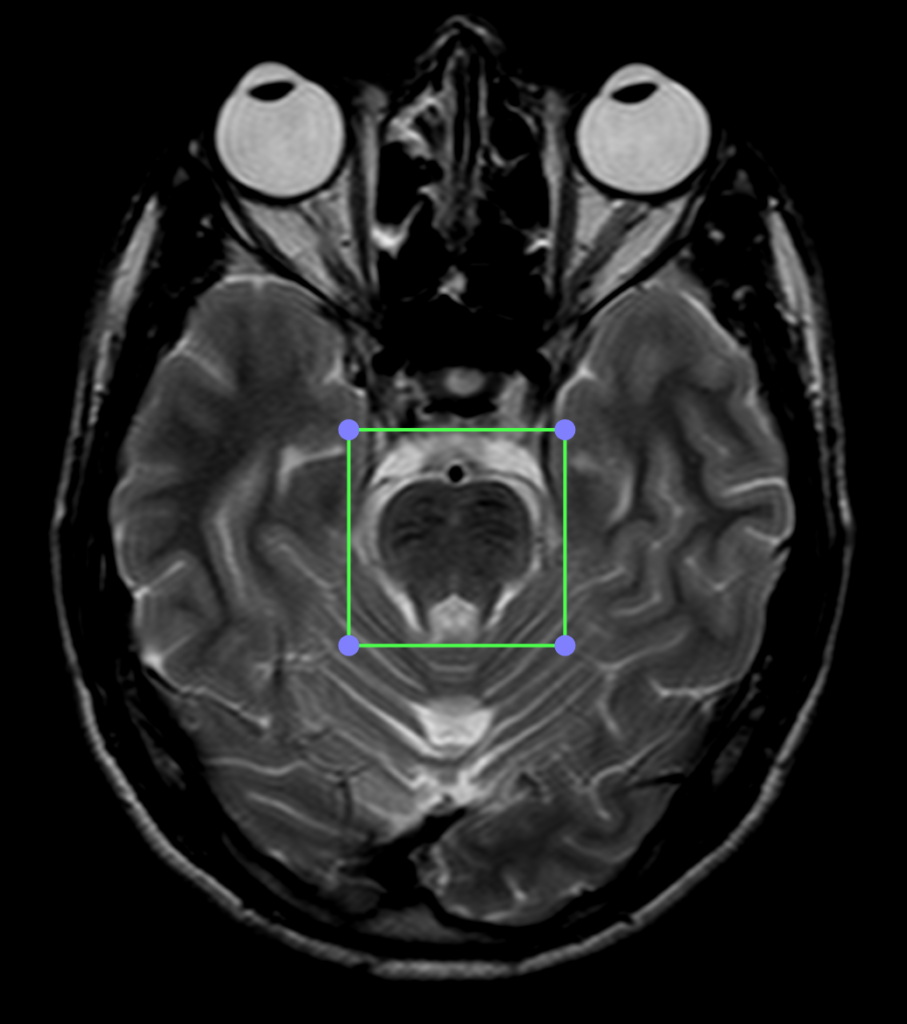
Case study: T2 hypointensity noted in the pons and midbrain region with mild reduction in the bulk of the vermis. Mild prominence of the cisterna magna noted. The cerebellar foliae appears mildly prominent. Long TR hyperintensities noted in the white matter regions of the corona radiata and centrum semiovale with no abnormality on the T1WI.
Images:
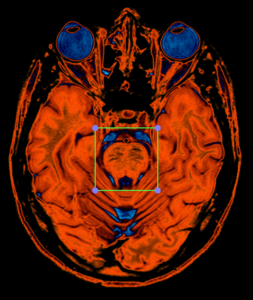
PERFUSION CLUT VIEW
T2WI Enlarged view of pons showing linear hypointensities.
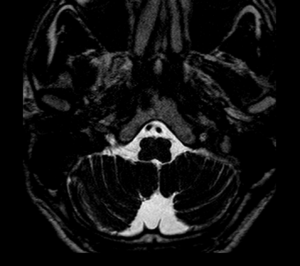
T2WI Heavy Weighted sequence shows prominent cisterna magna.
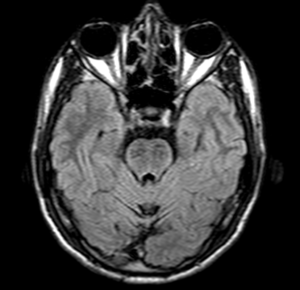
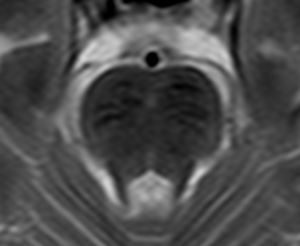
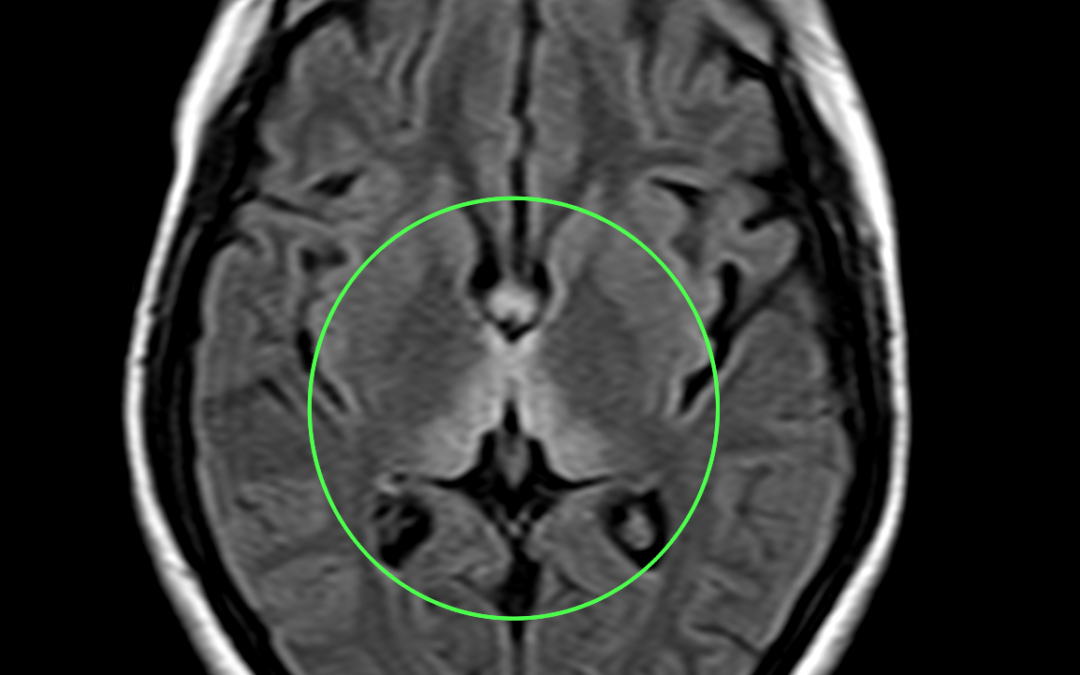
FLAIR shows hypointense linear areas on pons.
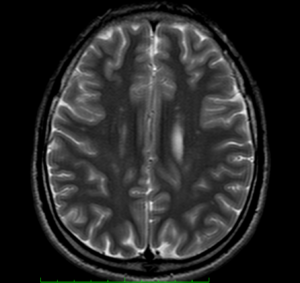
T2WI shows hyperintense scattered and confluent areas involving corona radiata and centrum semiovale.
Conclusion : K/c/o spastic ataxia and progressive walking difficulty follow up;T2 hypointensities in the region of the midbrain and pons with reduced bulk of the vermis and prominence of the cerebellar foliae.
Reference :
- https://radiopaedia.org/articles/autosomal-recessive-spastic-ataxia-of-charlevoix-saguenay-1
- 2.De michele G, Filla A. Other autosomal recessive and childhood ataxias. Handb Clin Neurol. 2012;103 : 343-57. doi:10.1016/B978-0-444-51892-7.00021-8 – Pubmed citation.
- Anheim M, Fleury M, Monga B et-al. Epidemiological, clinical, paraclinical and molecular study of a cohort of 102 patients affected with autosomal recessive progressive cerebellar ataxia from Alsace, Eastern France: implications for clinical management. Neurogenetics. 2010;11 (1): 1-12. doi:10.1007/s10048-009-0196-y – Pubmed citation
by Nithesh Ravindran | Aug 28, 2022
Age: 27yr
Sex: Female
Complaints: Gait ataxia and ophthalmoplegia confusion.
Case study: Areas of symmetrical increased T2/FLAIR signal seen involving dorsomedial thalami, tectal plate, periaqueductal area, around 3rd ventricle, mammillary bodies, posterior medulla (in medial vestibular nuclei and hypoglossal nuclei) with corresponding subtle diffusion restriction.
Images:
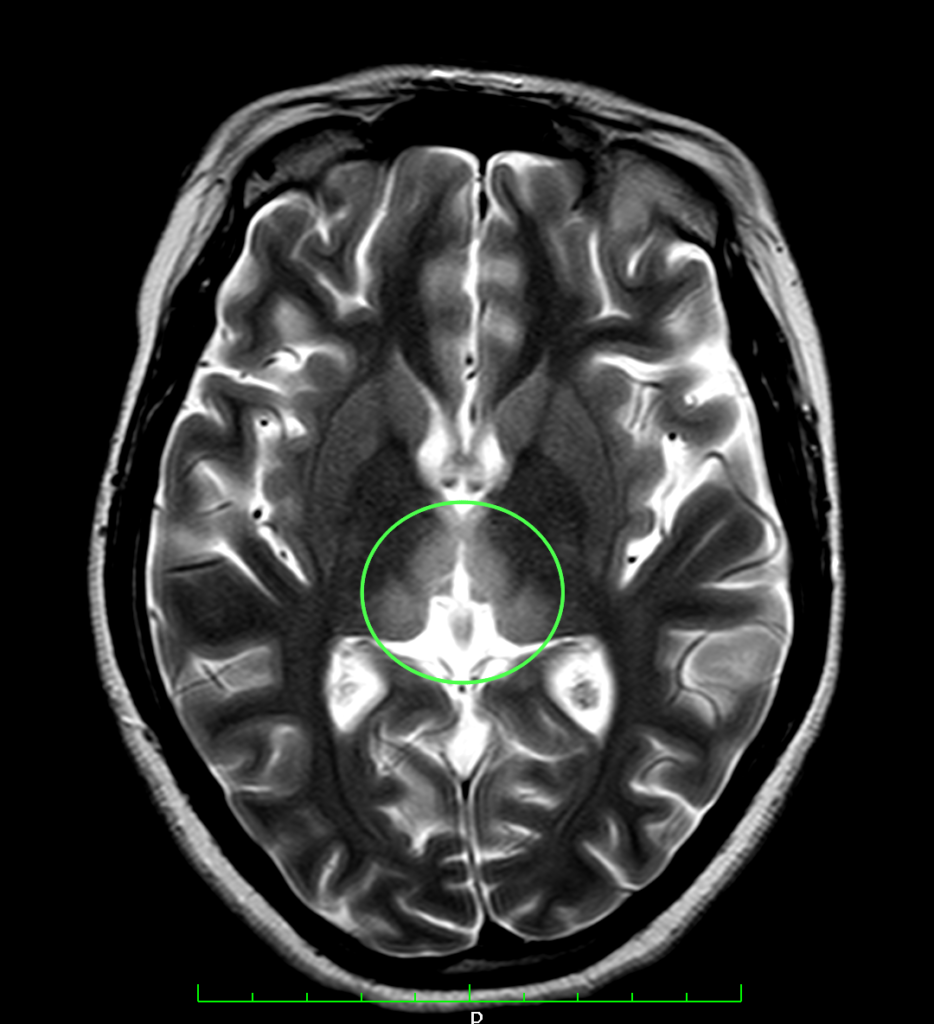
T2WI shows hyperintense signal involving dorsomedial aspect of thalamus.

FLAIR sequence shows hyperintensity involving the medial aspect of thalamus
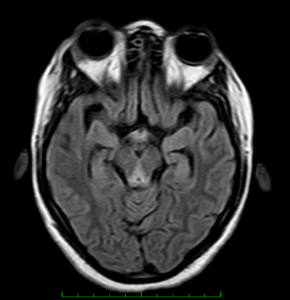
Conclusion : Imaging features suggestive of wernicke encephalopathy.