by Nithesh Ravindran | Oct 11, 2022
Age: 59yrs
Sex: Male
Complaints:
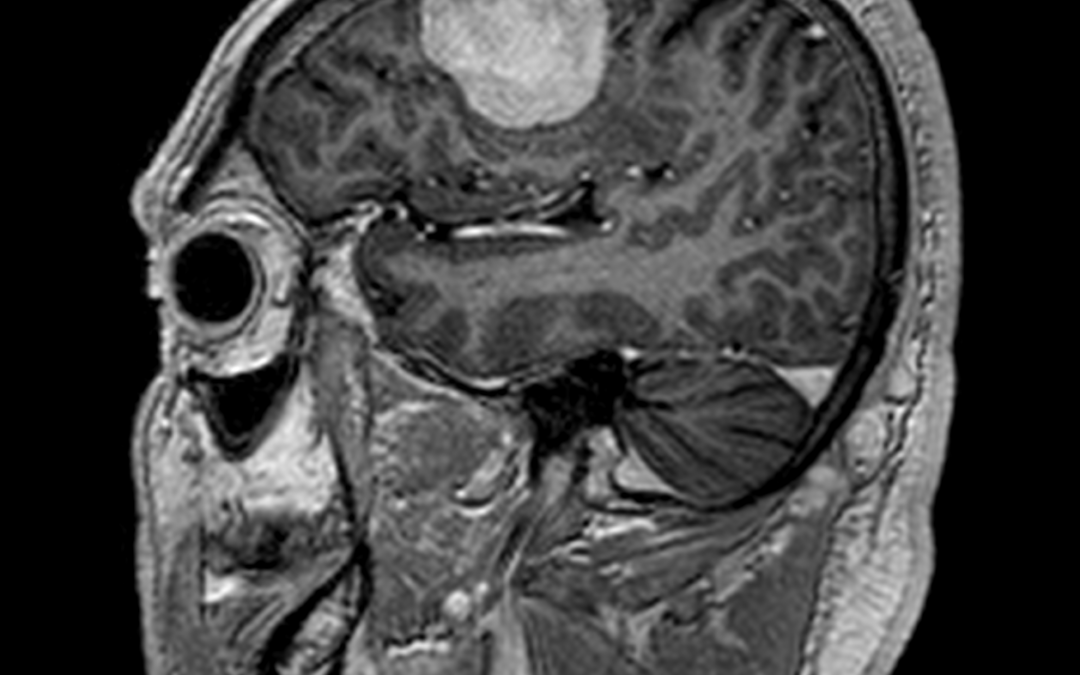
Case study: Supratentorial extra-axial dural based well defined lesion in right frontal convexity measuring 4.2 x 2.6 x 3.5 cm (AP x TR x CC) causing moderate perilesional edema and mild mass effect on adjacent brain parenchyma seen.
Dural tail and homogeneous vivid enhancement seen following contrast. The lesion appears iso intense to grey matter in T1WI and hyperintense in FLAIR/T2.
Images:
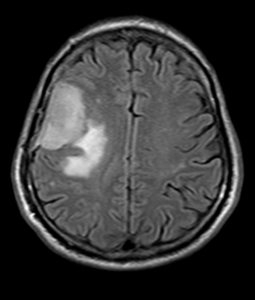
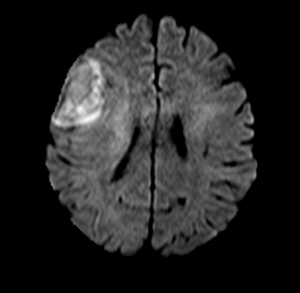

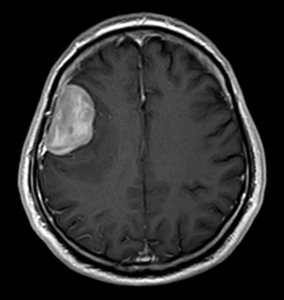
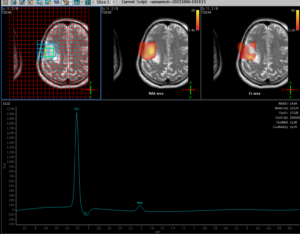
Conclusion :Extra-axial dural based vividly enhancing lesion in right frontal convexity causing moderate perilesional edema and mild mass effect – Imaging features favor meningioma.Mild diffusion restriction seen (hyperintense in DWI with intermediate signal in ADC). No blooming to suggest hemorrhage or calcification. MRS shows choline peak.
by Nithesh Ravindran | Oct 11, 2022
Age: 11 Yrs
Sex: Female
Complaints: Developmental abnormalities. K/c/o HIE.
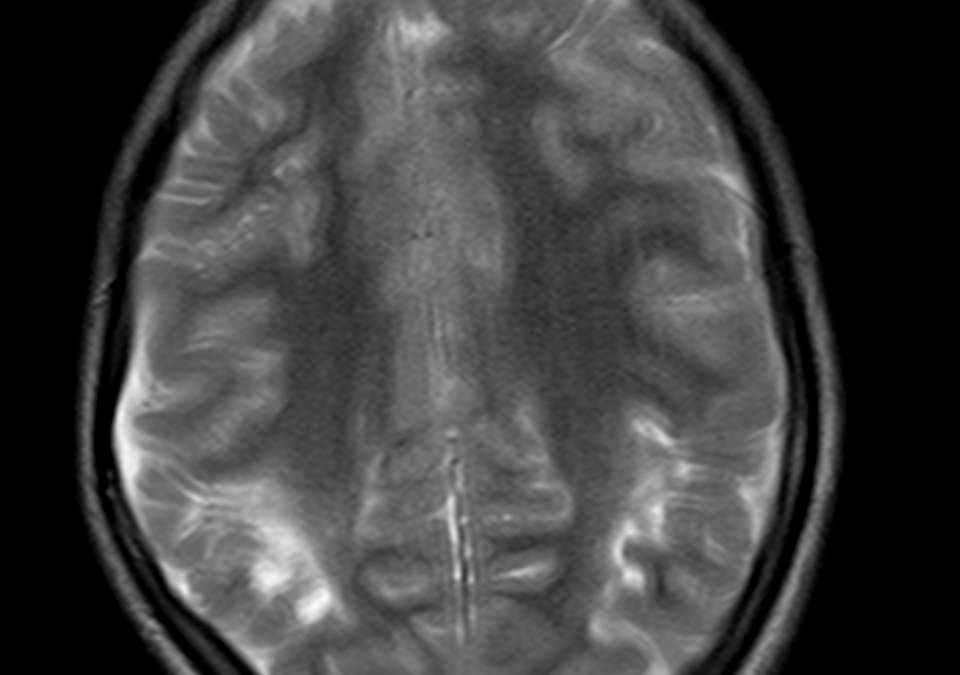
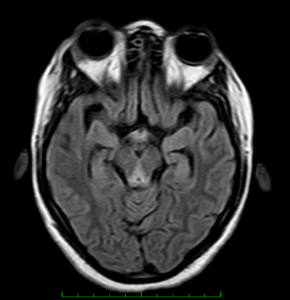
Case study: Evidence of periventricular T2/FLAIR hyperintensities seen in the posterior fossa around the occipital horn extending into the adjacent sulcal spaces. The corpus callosum shows significant thinning predominantly involving the isthmus and splenium. Volume loss seen in the right hippocampal head with widening of CSF space. There is asymmetric ex-vacuo dilatation of right occipital horn of lateral ventricle.
Images:
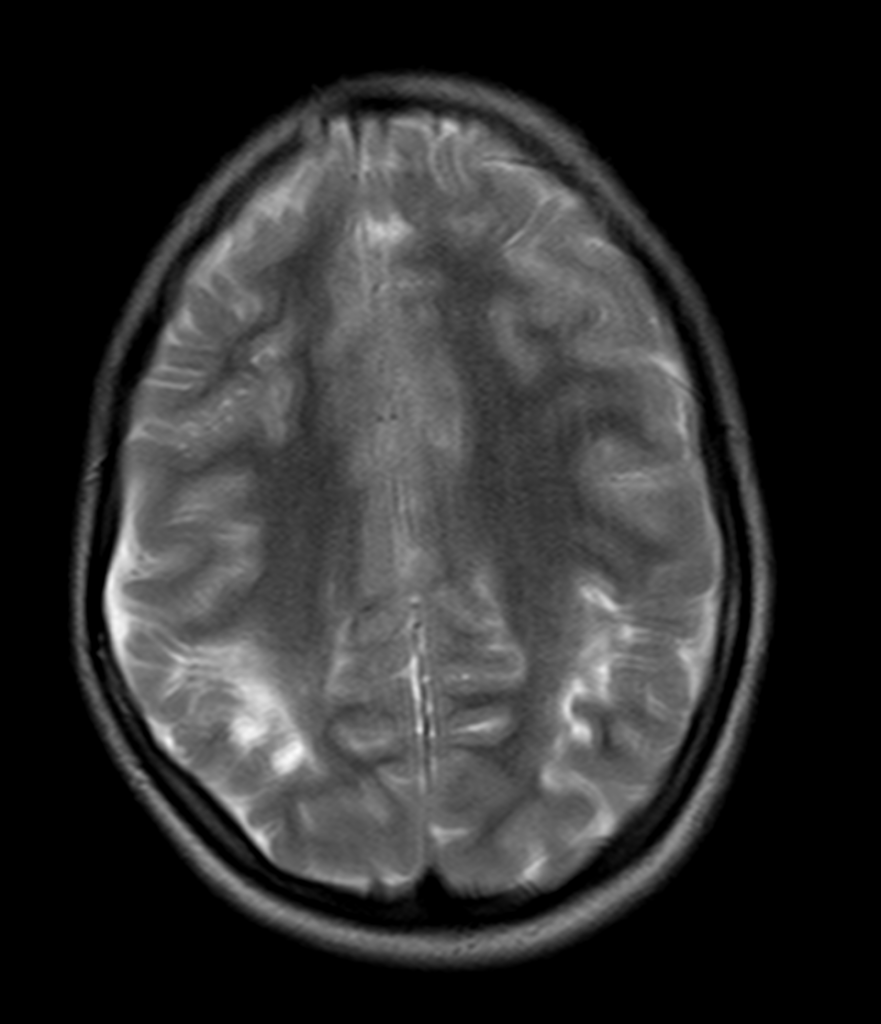



Conclusion: Atrophic changes involving the bilateral cerebral hemisphere in the form of periventricular and deep white matter hyperintensities showing cortical thinning along with asymmetric ex-vacuo dilatation of occipital horn. Corpus callosal thinning involving the isthmus and splenium. Right hippocampal volume loss. – Features are in consistent with atrophic changes as sequelae of Hypoxic Ischemic Encephalopathy.
by Nithesh Ravindran | Oct 11, 2022
Age: 48yr
Sex: Female
Complaints: Sudden headache and unconsciousness.
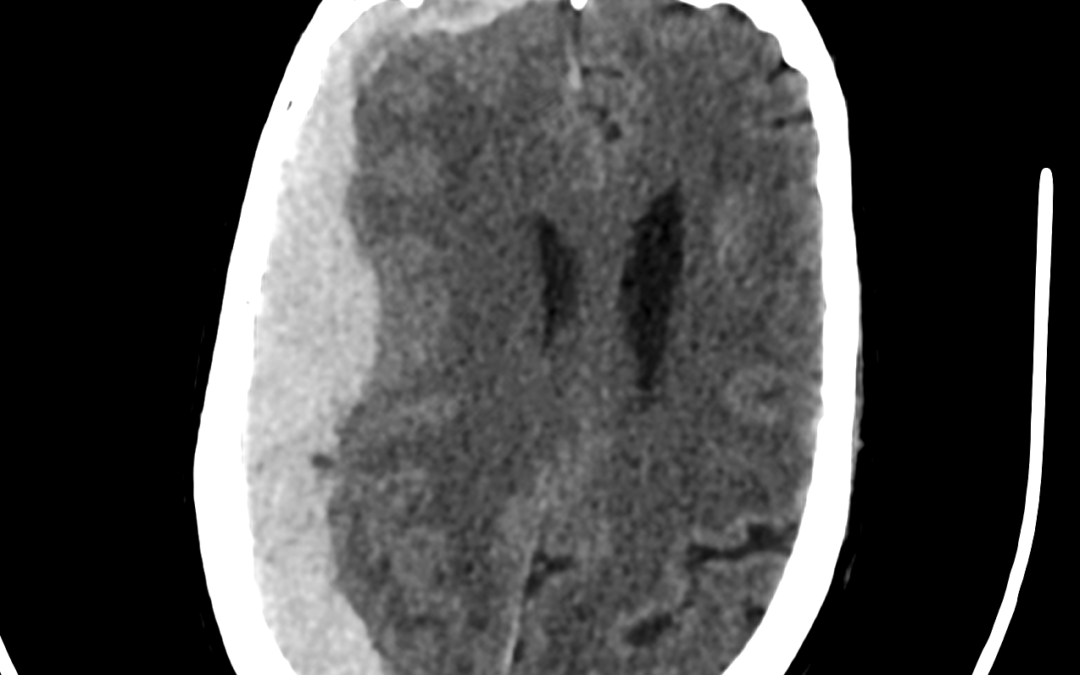
Case study: Extra axial, crescent shaped, hyperdense areas noted along the right temporo-fronto-parietal convexity (maximum thickness ~22 mm) causing mass effect in the form of effacement of ipsilateral sulcal spaces, compression of the ipsilateral lateral ventricle, subfalcine hernia and midline shift (~ 11mm) to the left.
Images:
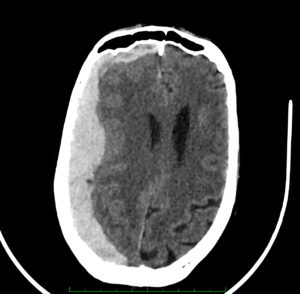
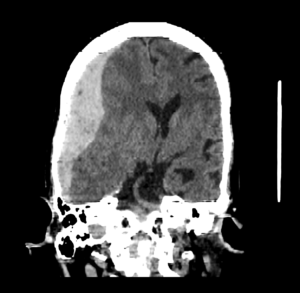

Conclusion: Subdural hemorrhage along the right tempero-fronto-parietal convexity causing mass effect and midline shift.
by Nithesh Ravindran | Aug 28, 2022
Age: 28yr
Sex: Male
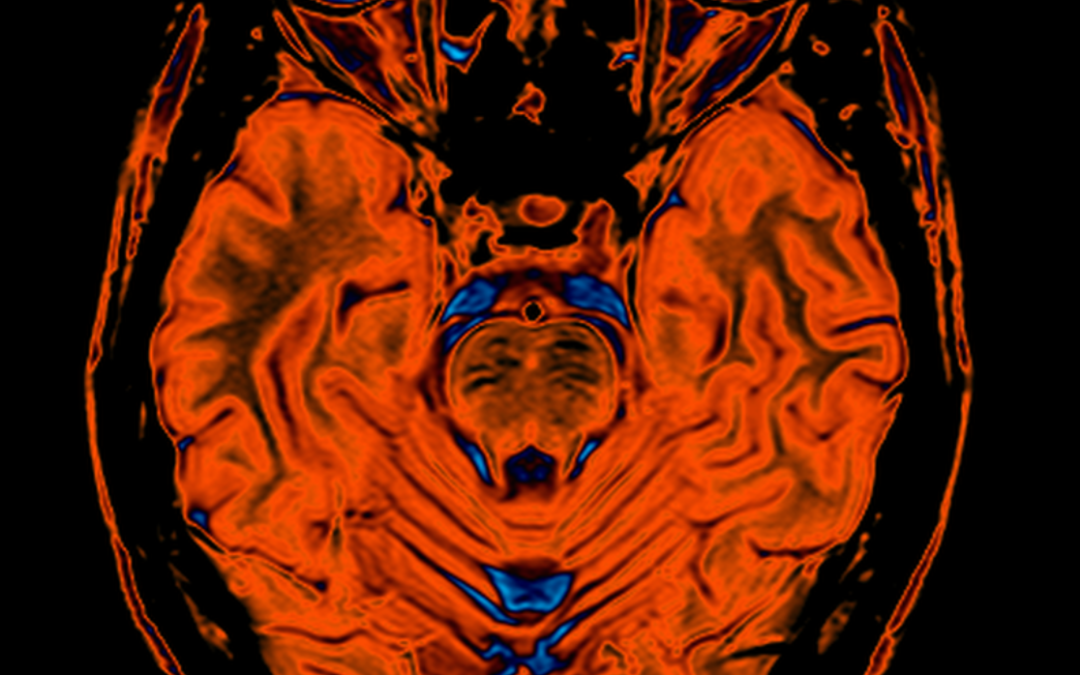
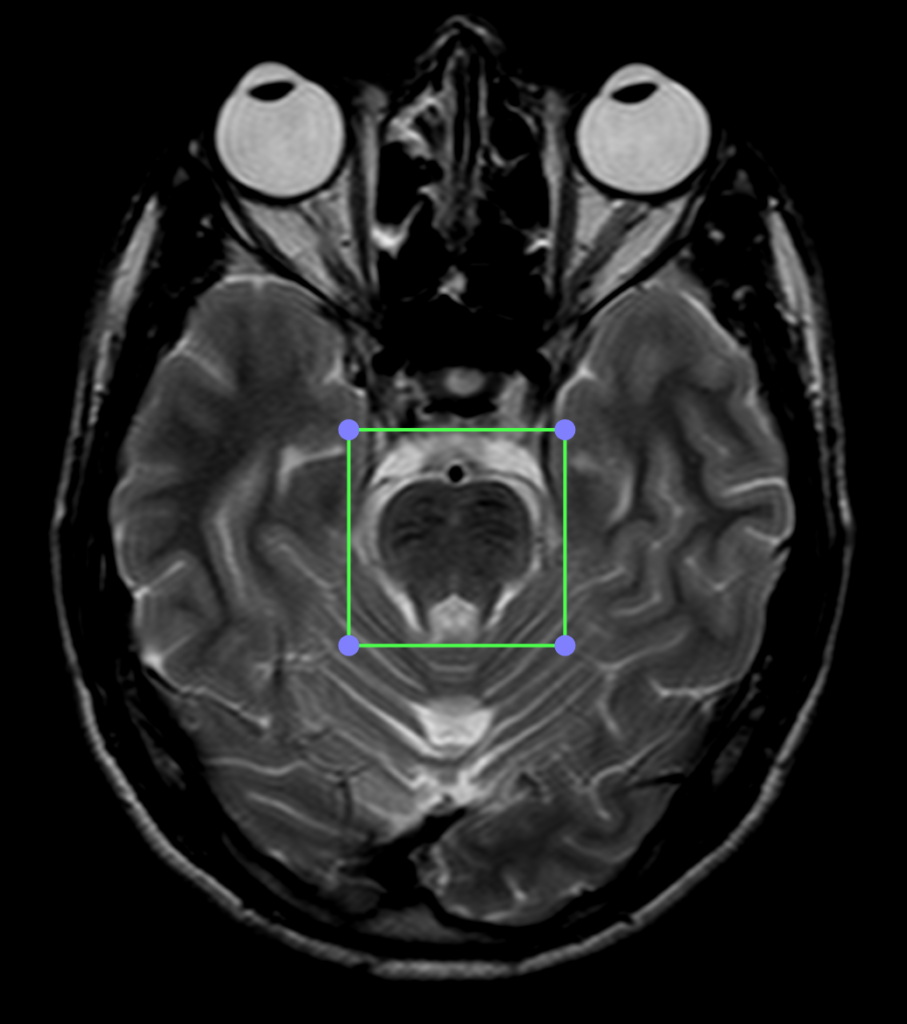
Complaints: Progressive walking difficulty.
Case study: T2 hypointensity noted in the pons and midbrain region with mild reduction in the bulk of the vermis. Mild prominence of the cisterna magna noted. The cerebellar foliae appears mildly prominent. Long TR hyperintensities noted in the white matter regions of the corona radiata and centrum semiovale with no abnormality on the T1WI.
Images:
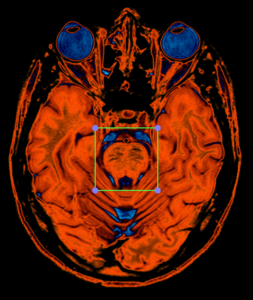
PERFUSION CLUT VIEW
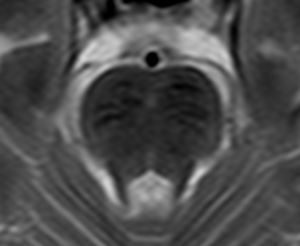
T2WI Enlarged view of pons showing linear hypointensities.
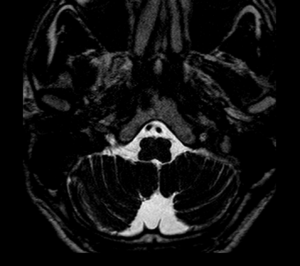
T2WI Heavy Weighted sequence shows prominent cisterna magna.
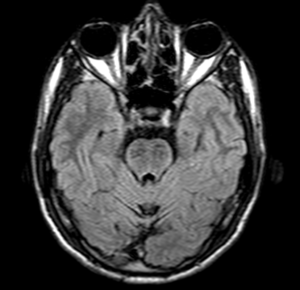
FLAIR shows hypointense linear areas on pons.
T2WI shows hyperintense scattered and confluent areas involving corona radiata and centrum semiovale.
Conclusion : K/c/o spastic ataxia and progressive walking difficulty follow up;T2 hypointensities in the region of the midbrain and pons with reduced bulk of the vermis and prominence of the cerebellar foliae.
Reference :
- https://radiopaedia.org/articles/autosomal-recessive-spastic-ataxia-of-charlevoix-saguenay-1
- 2.De michele G, Filla A. Other autosomal recessive and childhood ataxias. Handb Clin Neurol. 2012;103 : 343-57. doi:10.1016/B978-0-444-51892-7.00021-8 – Pubmed citation.
- Anheim M, Fleury M, Monga B et-al. Epidemiological, clinical, paraclinical and molecular study of a cohort of 102 patients affected with autosomal recessive progressive cerebellar ataxia from Alsace, Eastern France: implications for clinical management. Neurogenetics. 2010;11 (1): 1-12. doi:10.1007/s10048-009-0196-y – Pubmed citation
by Nithesh Ravindran | Aug 28, 2022
Age: 27yr
Sex: Female
Complaints: Gait ataxia and ophthalmoplegia confusion.
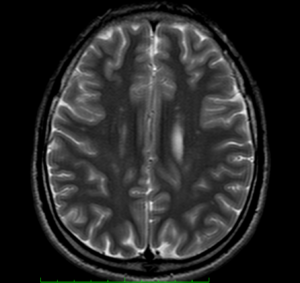
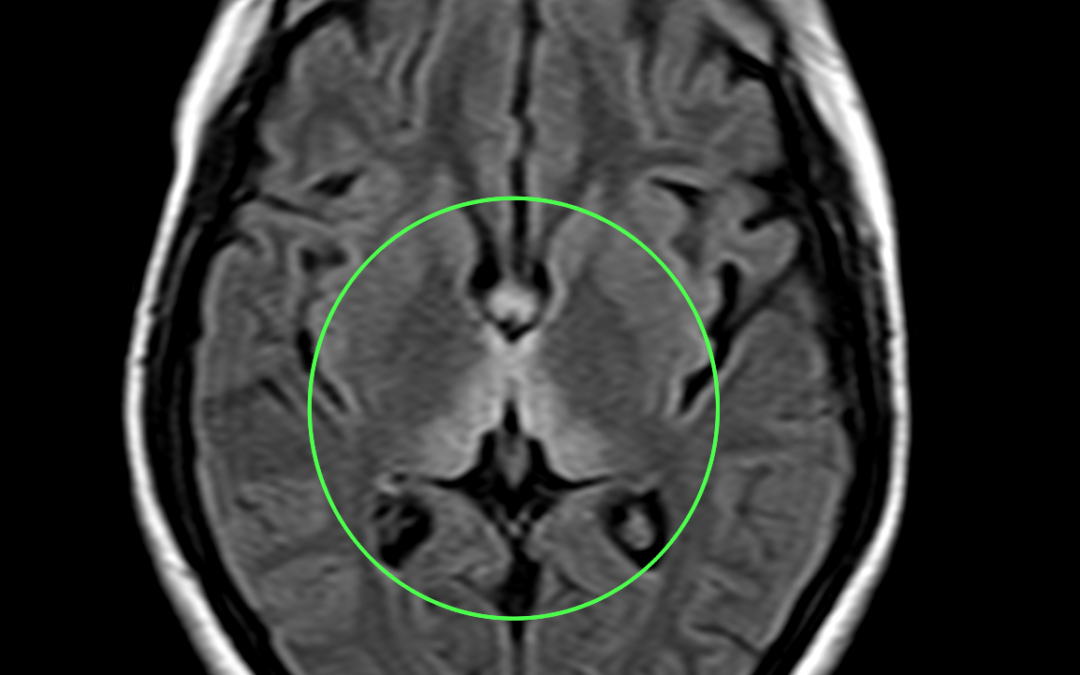
Case study: Areas of symmetrical increased T2/FLAIR signal seen involving dorsomedial thalami, tectal plate, periaqueductal area, around 3rd ventricle, mammillary bodies, posterior medulla (in medial vestibular nuclei and hypoglossal nuclei) with corresponding subtle diffusion restriction.
Images:
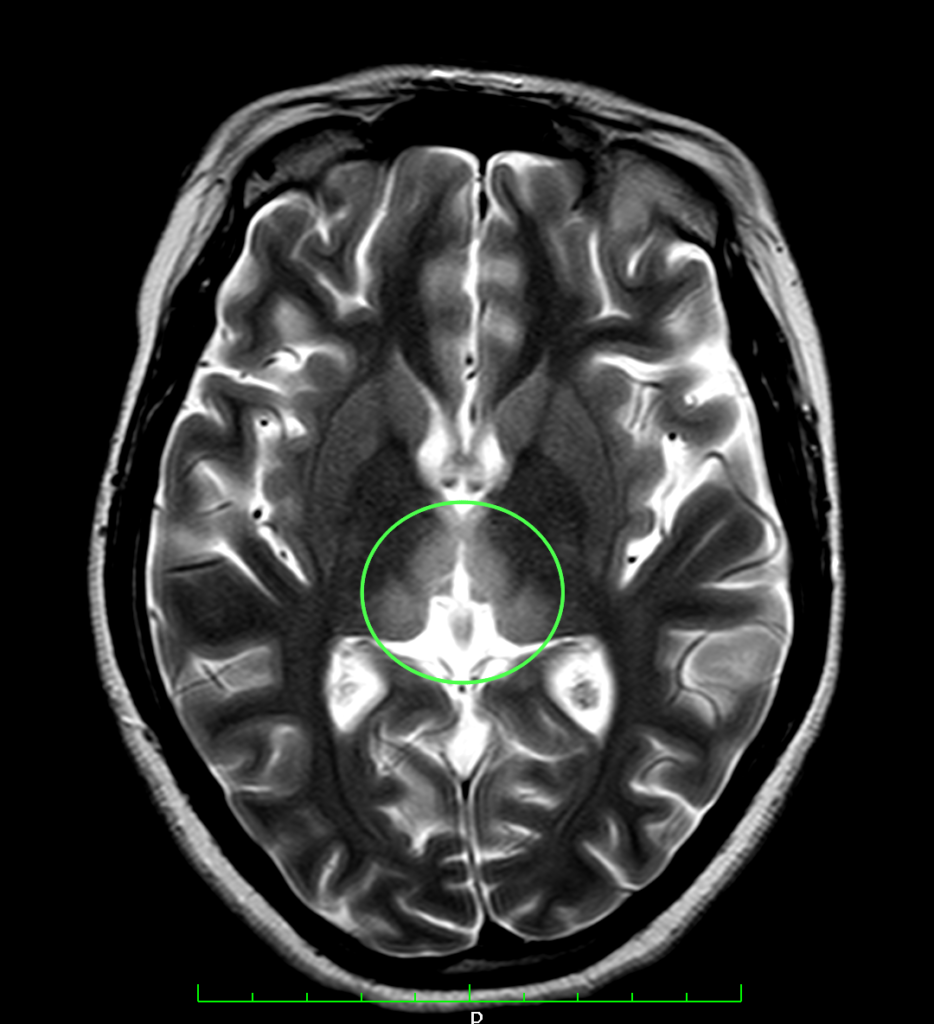
T2WI shows hyperintense signal involving dorsomedial aspect of thalamus.

FLAIR sequence shows hyperintensity involving the medial aspect of thalamus
Conclusion : Imaging features suggestive of wernicke encephalopathy.
by Nithesh Ravindran | Aug 28, 2022
Age: 74yr
Sex: Female
Complaints: Left limb weakness.
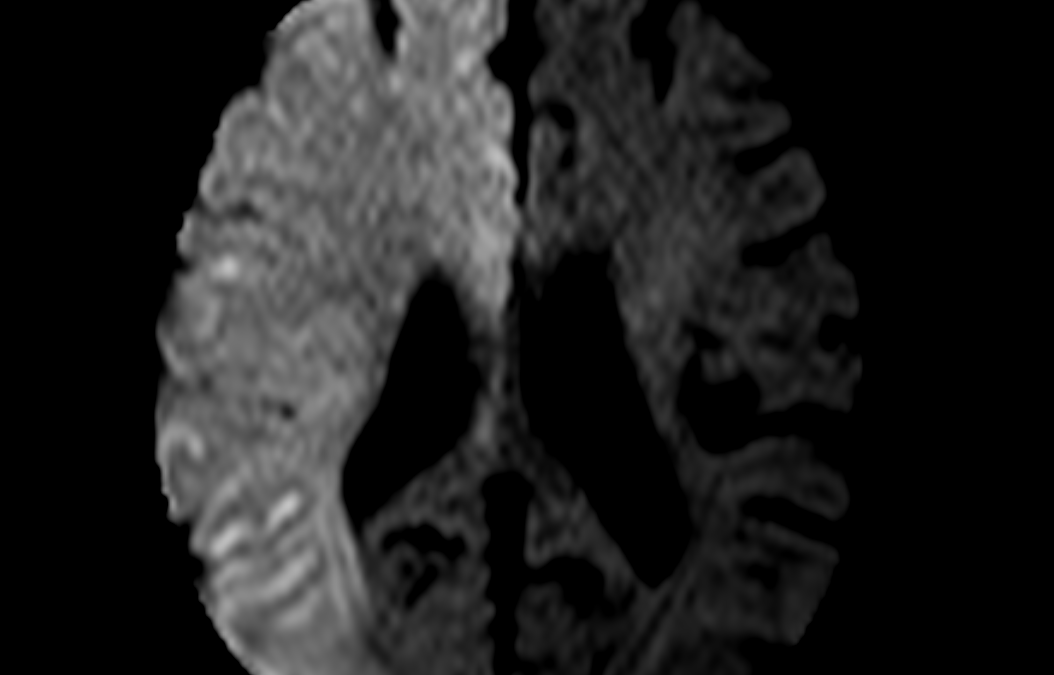
Case study: Large area of diffusion restriction with corresponding low ADC signal seen involving right fronto- parieto- temporal lobe with no signal abnormalities in corresponding T2 and FLAIR sequence.Angiography study shows non-visualisation right internal carotid artery (ICA) and its branches.No evidence of blooming in GRE sequence.
Images:
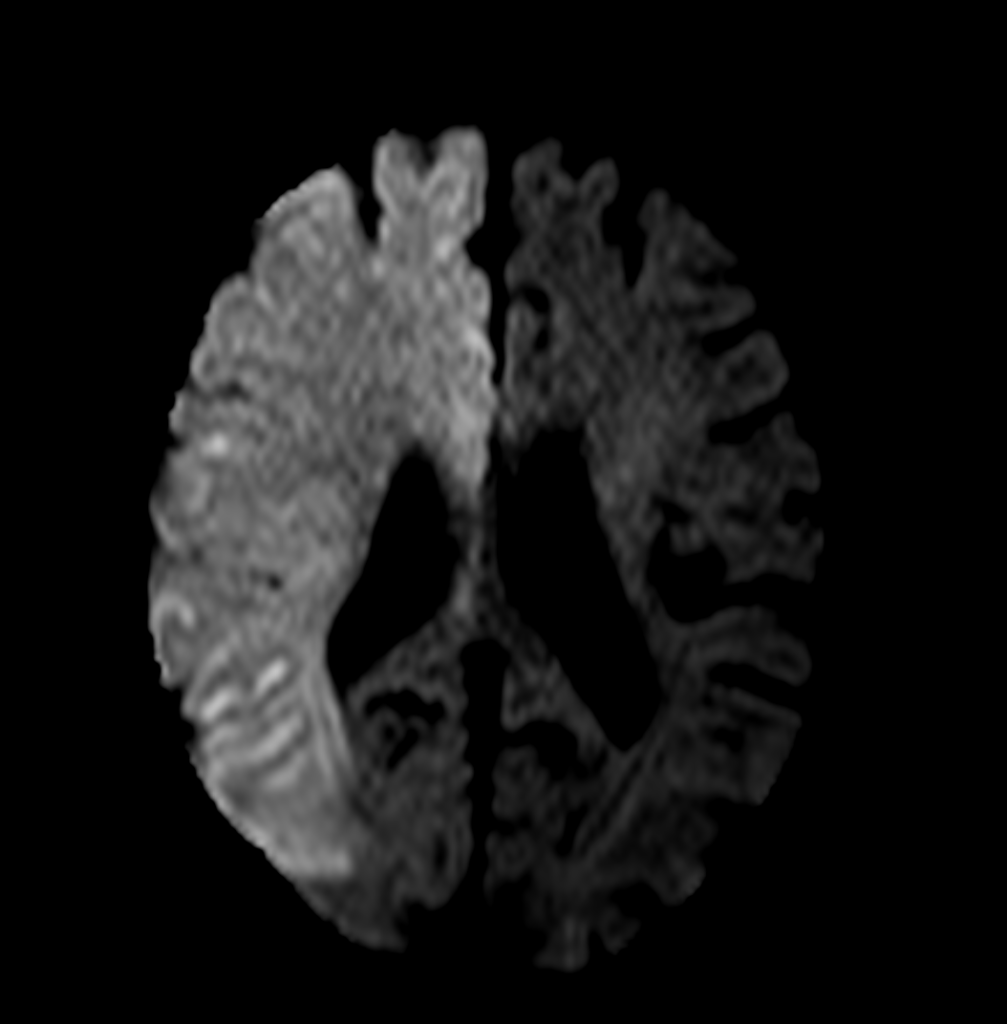
DWI
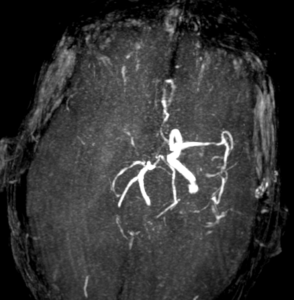
Angiography
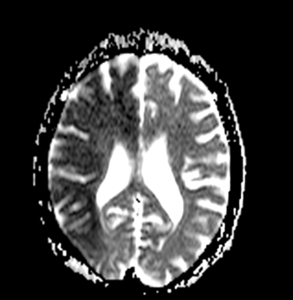
ADC
Conclusion :
- Acute infract involving right MCA and ACA territory.
- Mild atrophic changes in brain.
- MR angiogram (cerebral angiogram) shows non visualized right ICA and its main branches indicating significant thrombosis.
.