by Nithesh Ravindran | Aug 28, 2022
Age: 28yr
Sex: Male
Complaints: Progressive walking difficulty.
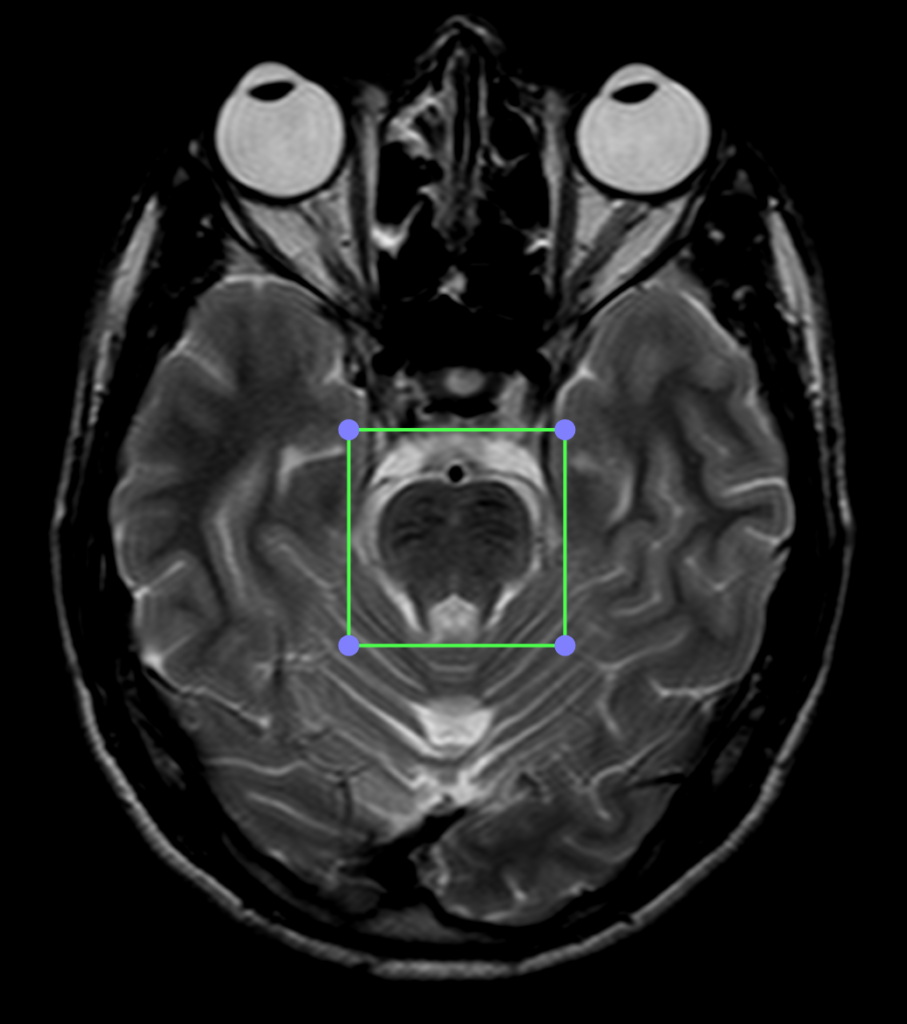
Case study: T2 hypointensity noted in the pons and midbrain region with mild reduction in the bulk of the vermis. Mild prominence of the cisterna magna noted. The cerebellar foliae appears mildly prominent. Long TR hyperintensities noted in the white matter regions of the corona radiata and centrum semiovale with no abnormality on the T1WI.
Images:
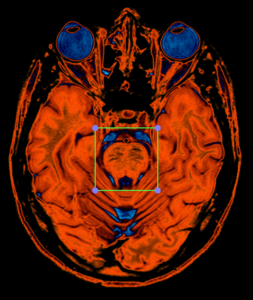
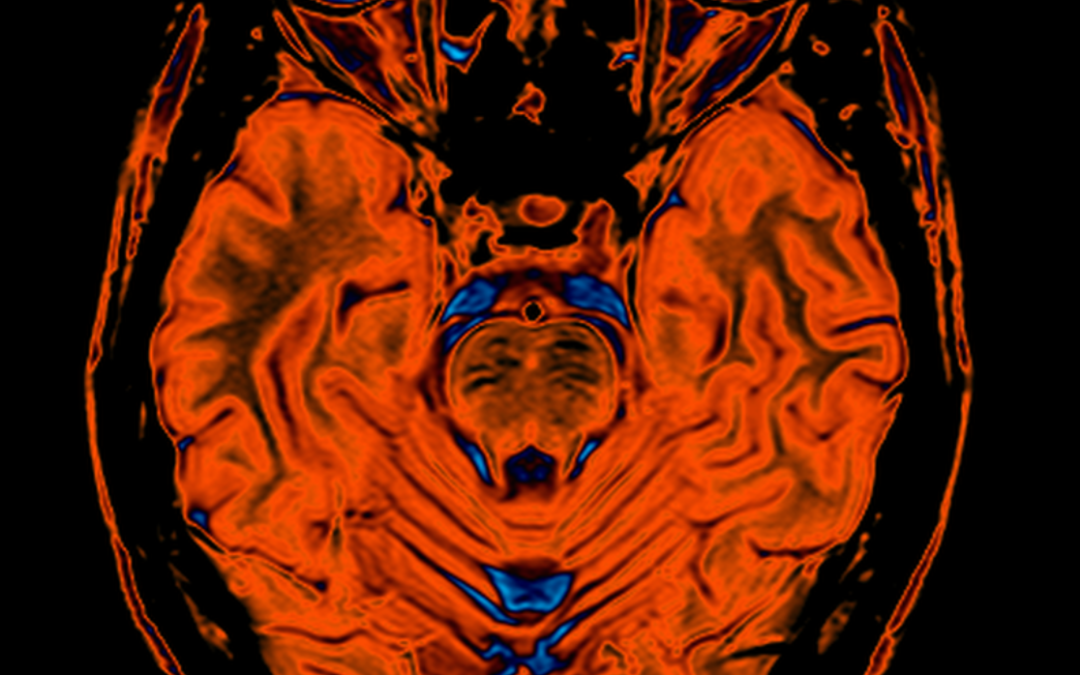
PERFUSION CLUT VIEW
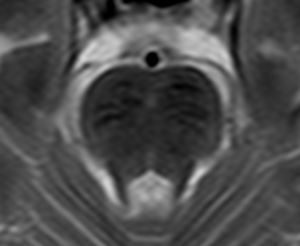
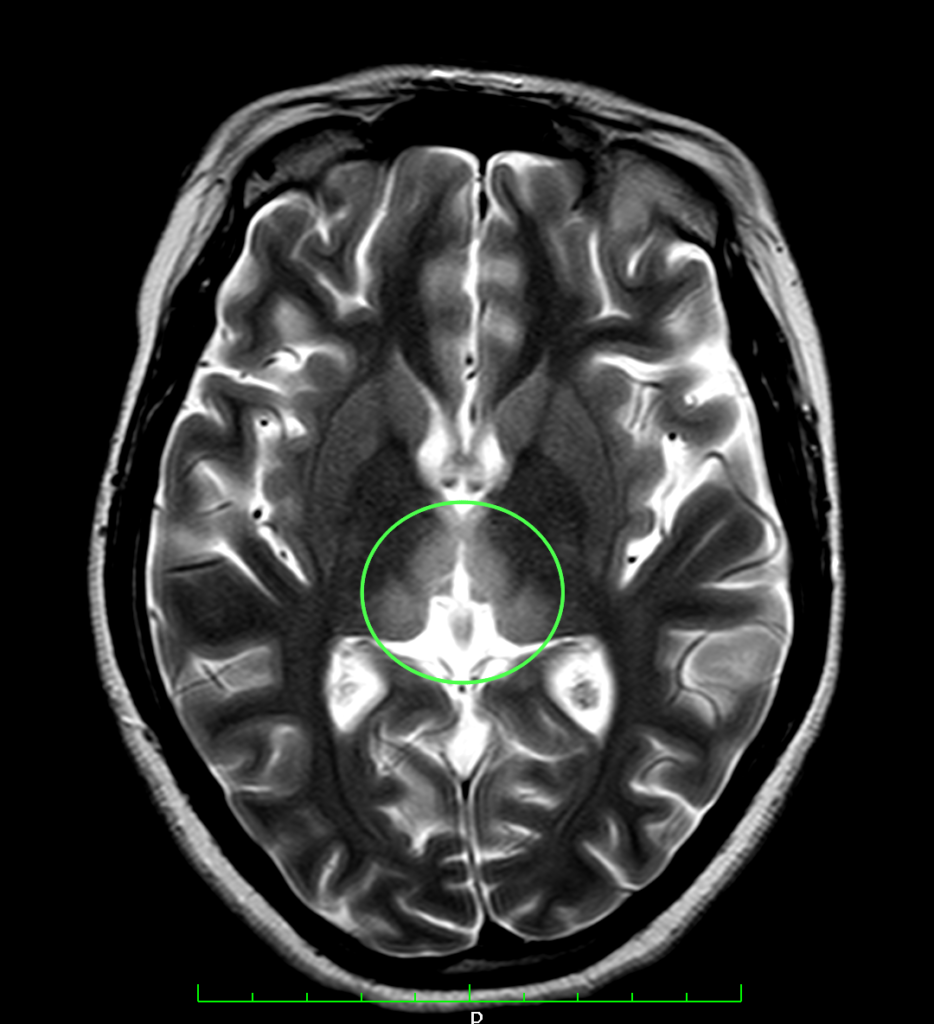
T2WI Enlarged view of pons showing linear hypointensities.
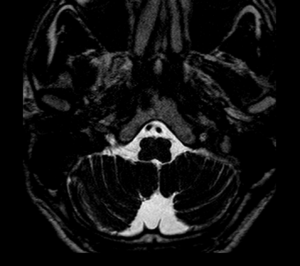
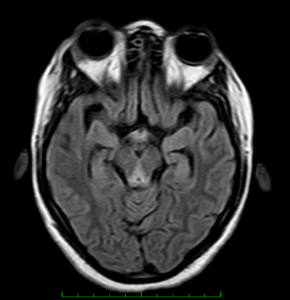
T2WI Heavy Weighted sequence shows prominent cisterna magna.
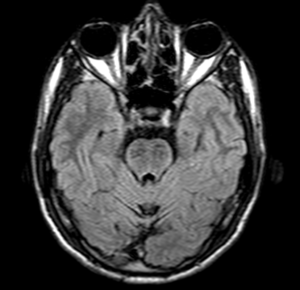
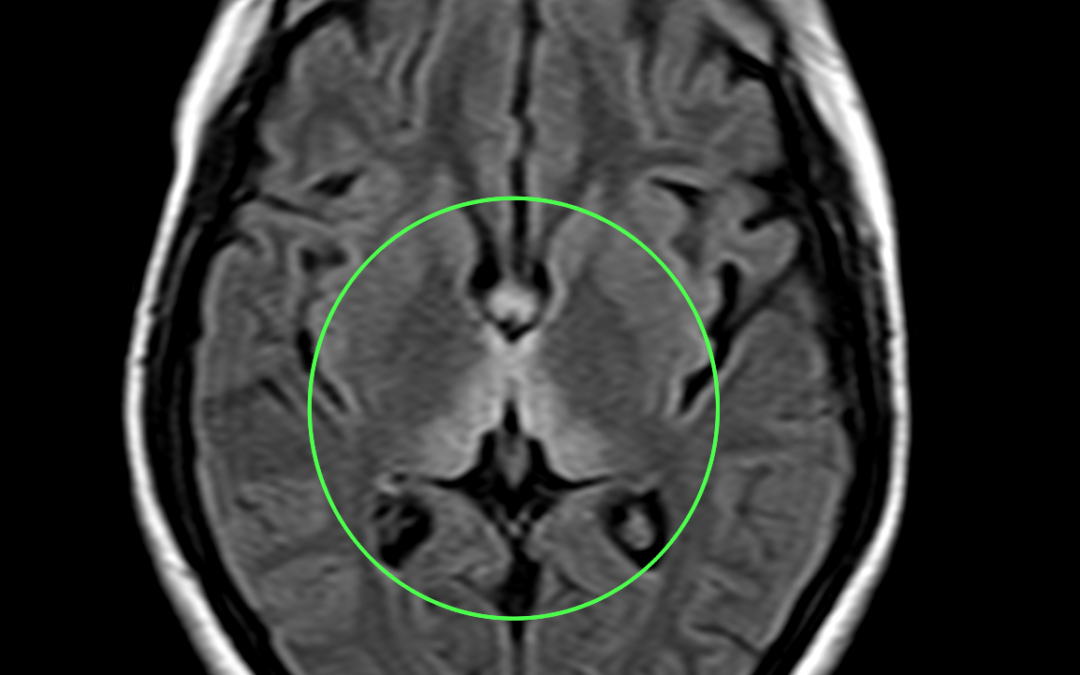
FLAIR shows hypointense linear areas on pons.
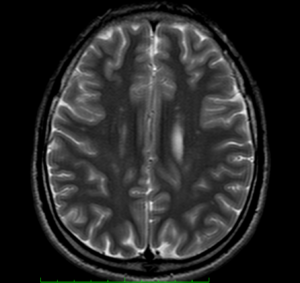
T2WI shows hyperintense scattered and confluent areas involving corona radiata and centrum semiovale.
Conclusion : K/c/o spastic ataxia and progressive walking difficulty follow up;T2 hypointensities in the region of the midbrain and pons with reduced bulk of the vermis and prominence of the cerebellar foliae.
Reference :
- https://radiopaedia.org/articles/autosomal-recessive-spastic-ataxia-of-charlevoix-saguenay-1
- 2.De michele G, Filla A. Other autosomal recessive and childhood ataxias. Handb Clin Neurol. 2012;103 : 343-57. doi:10.1016/B978-0-444-51892-7.00021-8 – Pubmed citation.
- Anheim M, Fleury M, Monga B et-al. Epidemiological, clinical, paraclinical and molecular study of a cohort of 102 patients affected with autosomal recessive progressive cerebellar ataxia from Alsace, Eastern France: implications for clinical management. Neurogenetics. 2010;11 (1): 1-12. doi:10.1007/s10048-009-0196-y – Pubmed citation
by Nithesh Ravindran | Aug 28, 2022
Age: 27yr
Sex: Female
Complaints: Gait ataxia and ophthalmoplegia confusion.
Case study: Areas of symmetrical increased T2/FLAIR signal seen involving dorsomedial thalami, tectal plate, periaqueductal area, around 3rd ventricle, mammillary bodies, posterior medulla (in medial vestibular nuclei and hypoglossal nuclei) with corresponding subtle diffusion restriction.
Images:
T2WI shows hyperintense signal involving dorsomedial aspect of thalamus.

FLAIR sequence shows hyperintensity involving the medial aspect of thalamus
Conclusion : Imaging features suggestive of wernicke encephalopathy.
by Nithesh Ravindran | Aug 28, 2022
Age: 74yr
Sex: Female
Complaints: Left limb weakness.
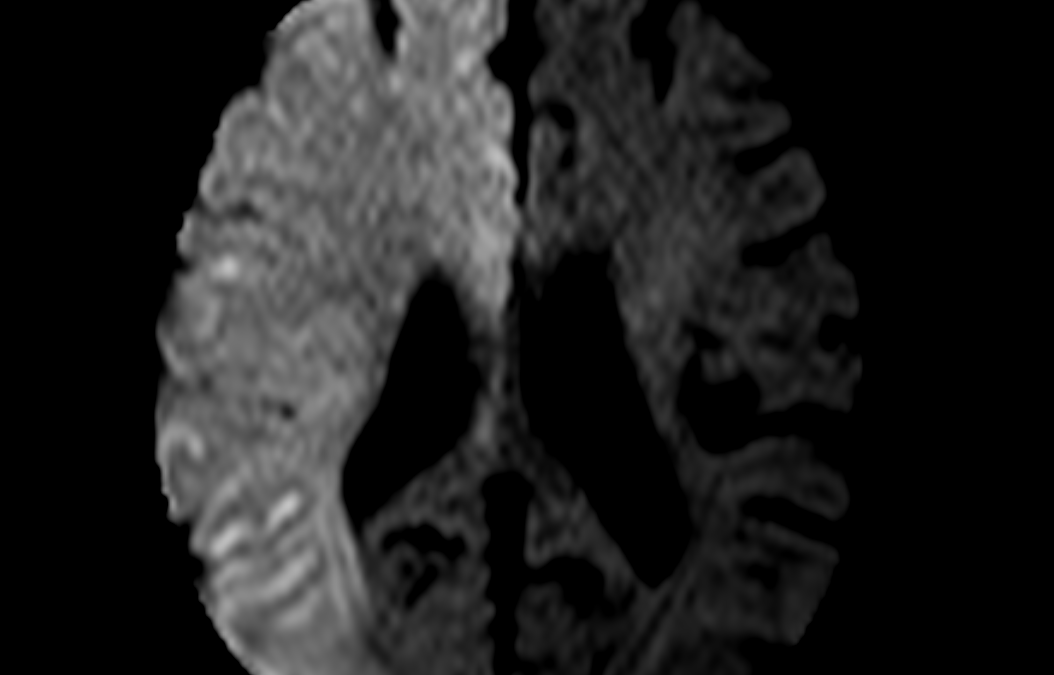
Case study: Large area of diffusion restriction with corresponding low ADC signal seen involving right fronto- parieto- temporal lobe with no signal abnormalities in corresponding T2 and FLAIR sequence.Angiography study shows non-visualisation right internal carotid artery (ICA) and its branches.No evidence of blooming in GRE sequence.
Images:
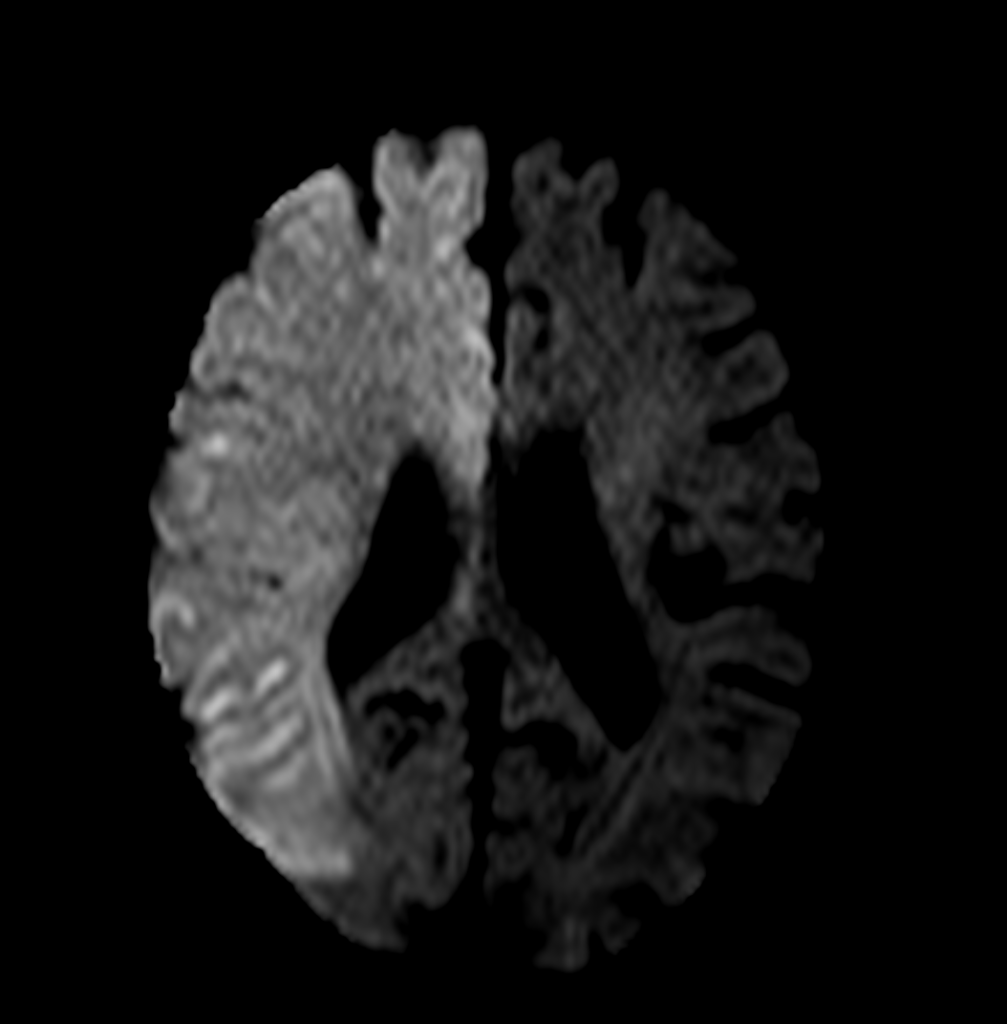
DWI
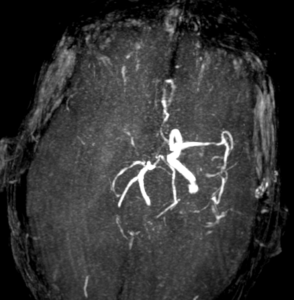
Angiography
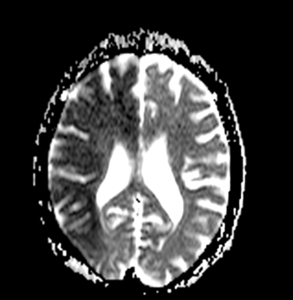
ADC
Conclusion :
- Acute infract involving right MCA and ACA territory.
- Mild atrophic changes in brain.
- MR angiogram (cerebral angiogram) shows non visualized right ICA and its main branches indicating significant thrombosis.
.
by Nithesh Ravindran | Aug 24, 2022
Age: 41 Yrs
Sex: Female
Complaints: Right lower abdominal pain.
Images:

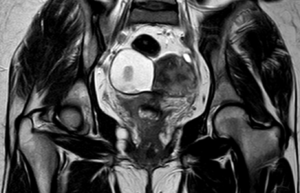
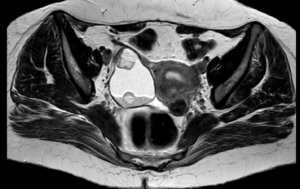

Case study: A large heterogenous exophytic lesion measuring 6.3 x 4.9 cm seen in the right adnexa derived from the ovary showing T1 & T2 hyperintense signal intensity and suppression in the STIR sequences. The lesion exhibits irregular solid nodular areas within. Other findings – leiomyomas.
Conclusion: Right adnexal lesion showing typical MRI features of T1/T2 hyperintensity and loss of signal in Fat suppressed sequences with nodular areas suggesting fat contents. – Dermoid cyst of the ovary. Variant – Matured cystic teratoma.
Reference : 1.https://radiopaedia.org/articles/mature-cystic-ovarian-teratoma-1 Mature cystic teratomas are encapsulated tumors with mature tissue or organ components. They are composed of well-differentiated derivations from at least two of the three germ cell layers (i.e. ectoderm, mesoderm, and endoderm). They, therefore, contain developmentally mature skin complete with hair follicles and sweat glands, sometimes luxuriant clumps of long hair, and often pockets of sebum, blood, fat (93%) 10, bone, nails, teeth, eyes, cartilage, and thyroid tissue. Typically their diameter is smaller than 10 cm, and rarely more than 15 cm. Real organoid structures (teeth, fragments of bone) may be present in ~30% of cases.
by Nithesh Ravindran | Dec 16, 2021
Age: 48 Yrs
Sex: Female
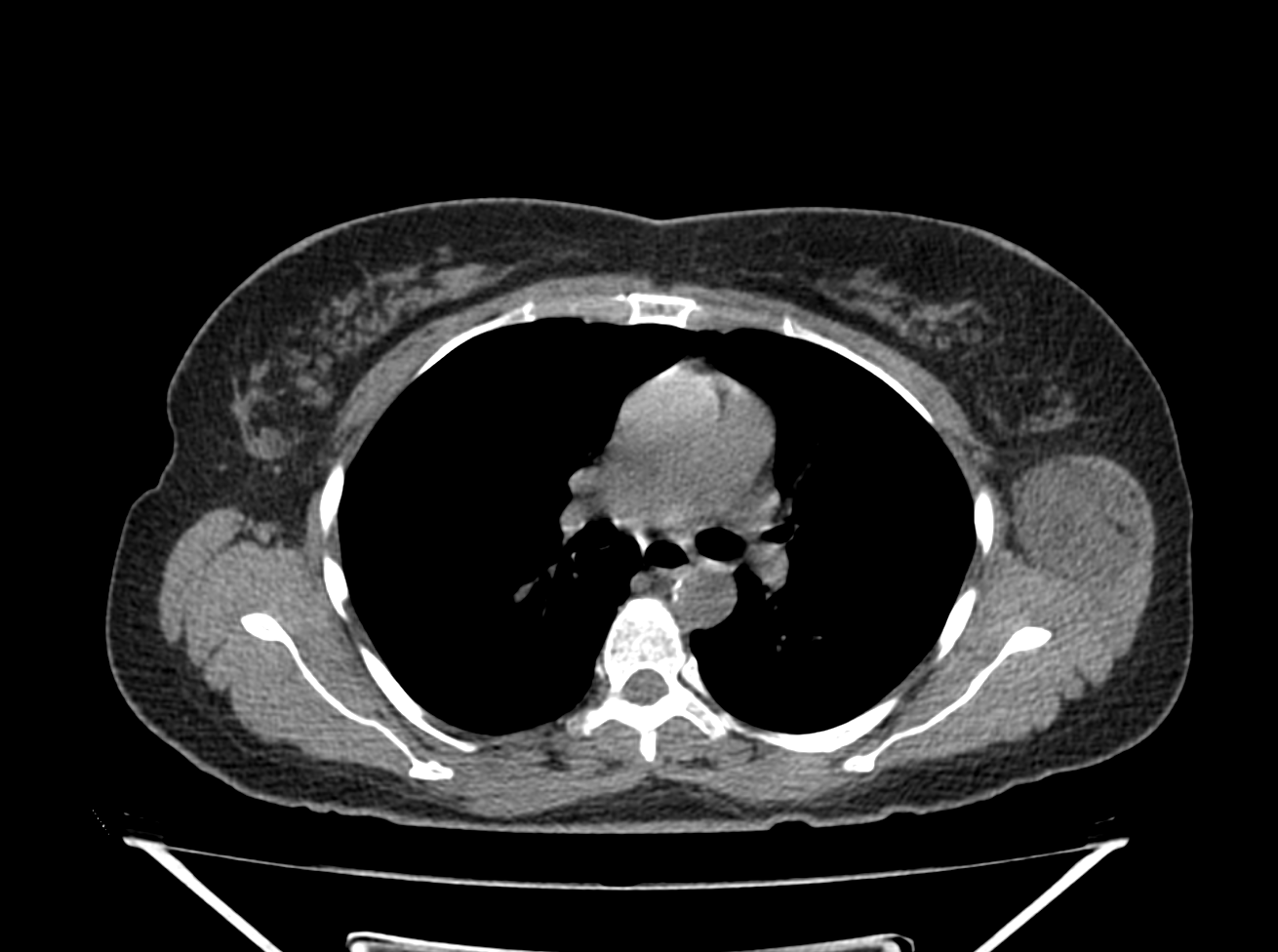
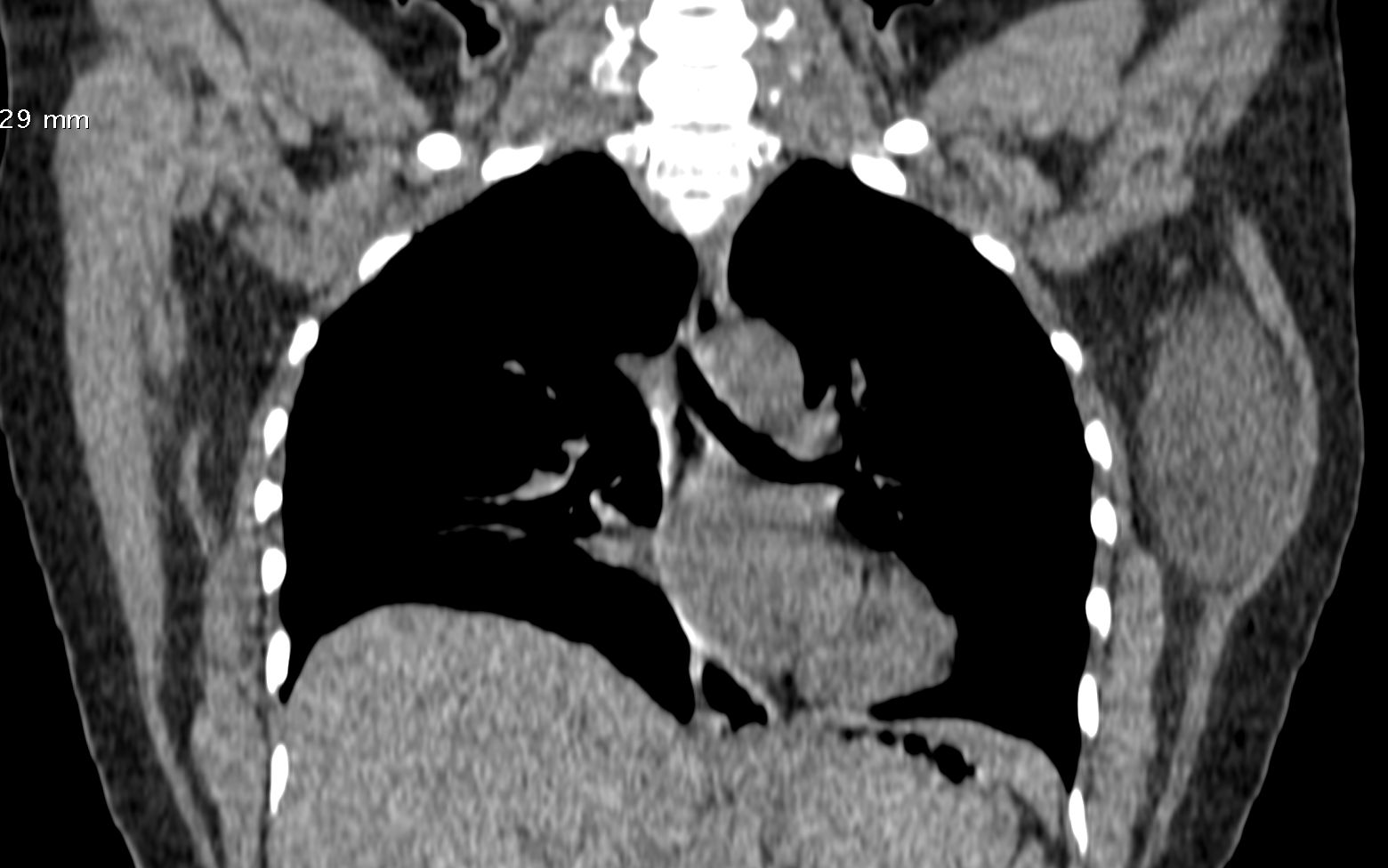
Complaints: H/o left chest wall swelling. No pain or skin abnormality.
Screen Shot 2021-12-15 at 19.37.26
Screen Shot 2021-12-15 at 19.38.33
Case Discussion :
Well defined smooth solid hypo to isodense lesion in the left chest wall seen arising from the latissimus dorsi muscle.
The is lesion is seen as a solid mass with hypo-dense attenuation, however the lesion shows typical fatty appearance.
The report was given as chest wall mass arising from left latissimus dorsi muscle.
Possible DD’s include: 1. Lipoma. 2. Schwannoma.