by Nithesh Ravindran | Oct 11, 2022
Age: 59yrs
Sex: Male
Complaints:
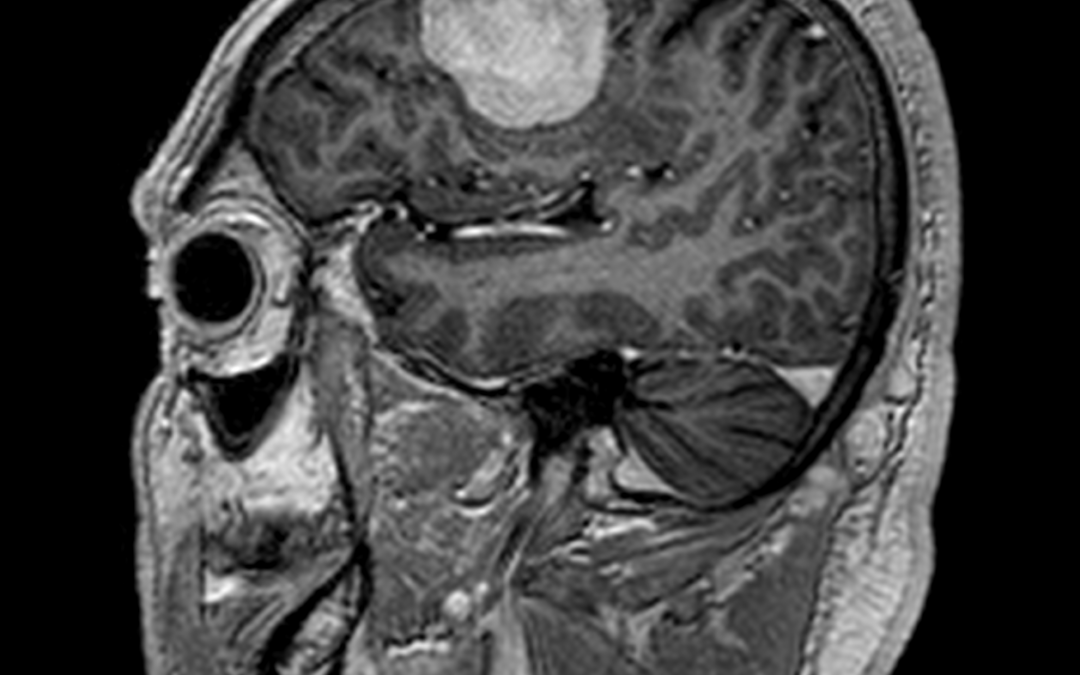
Case study: Supratentorial extra-axial dural based well defined lesion in right frontal convexity measuring 4.2 x 2.6 x 3.5 cm (AP x TR x CC) causing moderate perilesional edema and mild mass effect on adjacent brain parenchyma seen.
Dural tail and homogeneous vivid enhancement seen following contrast. The lesion appears iso intense to grey matter in T1WI and hyperintense in FLAIR/T2.
Images:
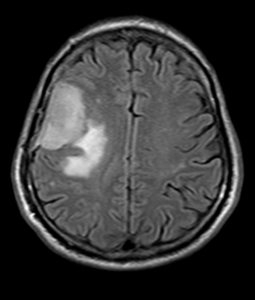
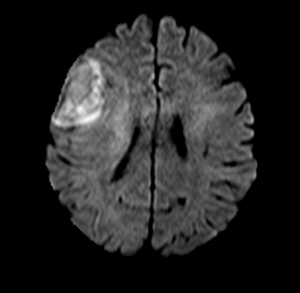

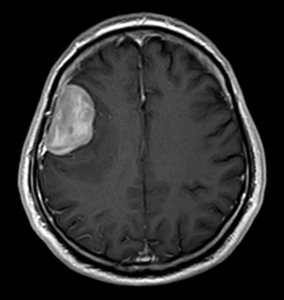
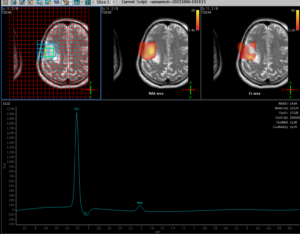
Conclusion :Extra-axial dural based vividly enhancing lesion in right frontal convexity causing moderate perilesional edema and mild mass effect – Imaging features favor meningioma.Mild diffusion restriction seen (hyperintense in DWI with intermediate signal in ADC). No blooming to suggest hemorrhage or calcification. MRS shows choline peak.
by Nithesh Ravindran | Oct 11, 2022
Age: 30Yrs
Sex: Male
Complaints: Pain on foot while walking.
Case study: Subchondral high signal noted in the mid aspect of the talus and the calcaneum with small subchondral cystic areas – Apparent on the STIR sequences. Evidence of osteophytic changes with cortical irregularity and narrowing of the talo-calcaneal joint anteriorly. The osteophyte is seen encroaching into the sinus tarsi with narrowing.
The tibio-calcaneal angle (kites angle) is 83 degrees – Normal.
The talo-calcaneal angle is 45 degrees – Abnormal.
Images:
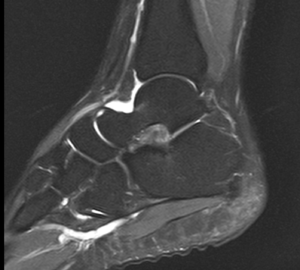
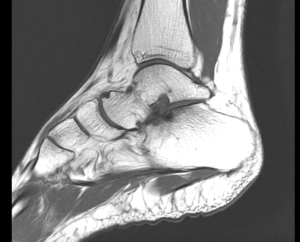
Conclusion : Subchondral talo-calcaneal high marrow signals with anterior joint space narrowing, osteophytic formation and encroachment into the sinus tarsi – Suggestive of talo-calcaneal impingement.
Increased talo-calcaneal angle (45 degrees) – Hindfoot valgus.
Peroneus longus and brevis tenosynovitis.
by Nithesh Ravindran | Oct 11, 2022
Age: 41Yrs
Sex: Female
Case Study: Well-defined T2/STIR hyperintense signal cystic lesion in the postero-lateral aspect of vagina.
Images:

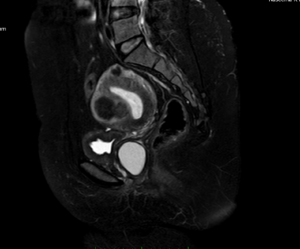
Conclusion : Postero-lateral wall of vagina shows a cyst as described – Suggestive of likely Bartholin’s cyst.
by Nithesh Ravindran | Oct 11, 2022
Age: 11 Yrs
Sex: Female
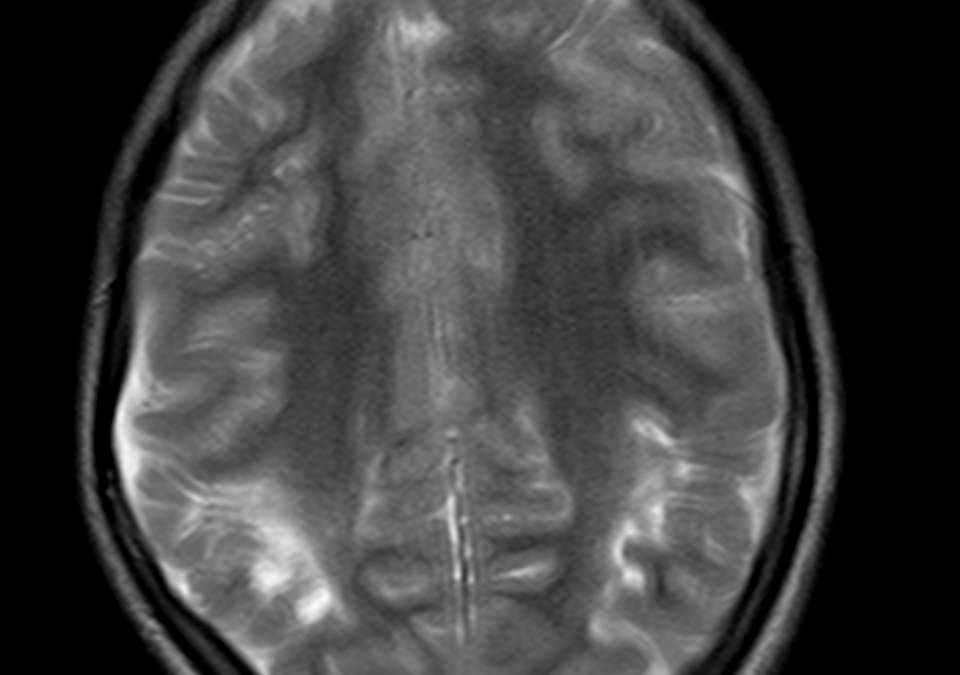
Complaints: Developmental abnormalities. K/c/o HIE.
Case study: Evidence of periventricular T2/FLAIR hyperintensities seen in the posterior fossa around the occipital horn extending into the adjacent sulcal spaces. The corpus callosum shows significant thinning predominantly involving the isthmus and splenium. Volume loss seen in the right hippocampal head with widening of CSF space. There is asymmetric ex-vacuo dilatation of right occipital horn of lateral ventricle.
Images:
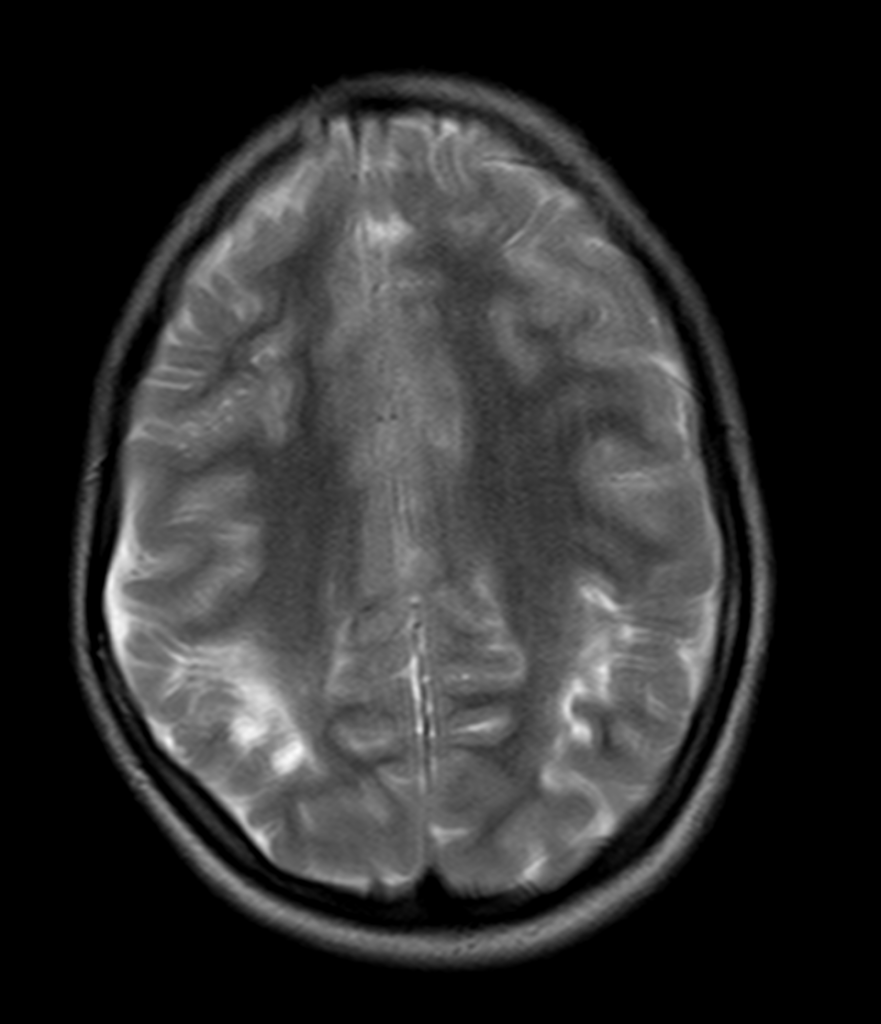



Conclusion: Atrophic changes involving the bilateral cerebral hemisphere in the form of periventricular and deep white matter hyperintensities showing cortical thinning along with asymmetric ex-vacuo dilatation of occipital horn. Corpus callosal thinning involving the isthmus and splenium. Right hippocampal volume loss. – Features are in consistent with atrophic changes as sequelae of Hypoxic Ischemic Encephalopathy.
by Nithesh Ravindran | Oct 11, 2022
Age: 48yr
Sex: Female
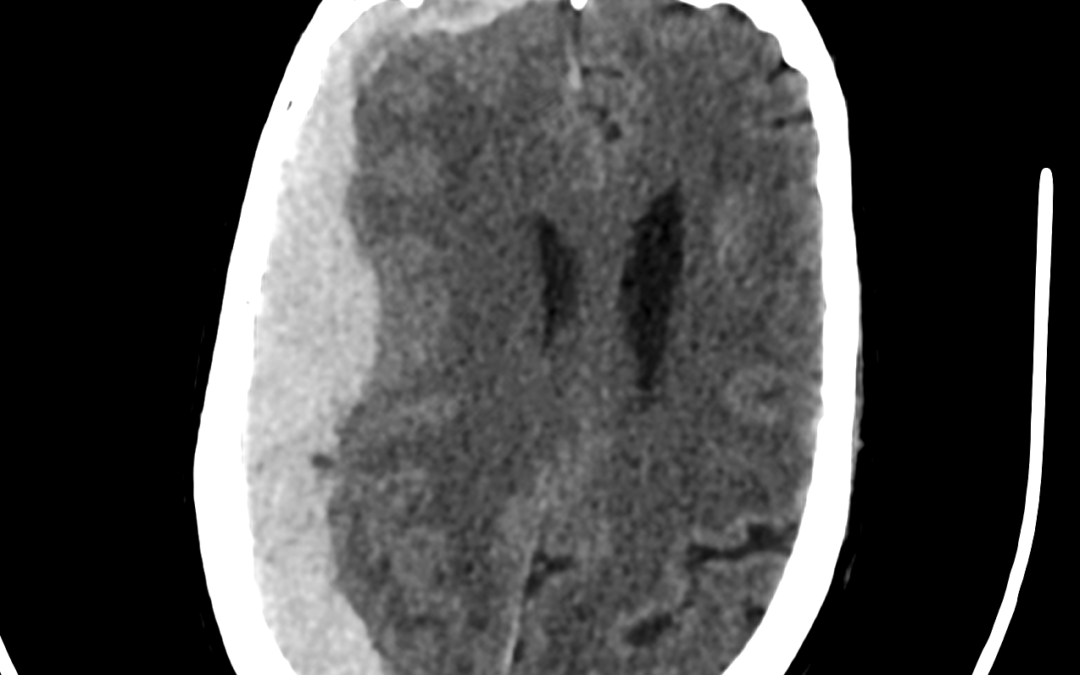
Complaints: Sudden headache and unconsciousness.
Case study: Extra axial, crescent shaped, hyperdense areas noted along the right temporo-fronto-parietal convexity (maximum thickness ~22 mm) causing mass effect in the form of effacement of ipsilateral sulcal spaces, compression of the ipsilateral lateral ventricle, subfalcine hernia and midline shift (~ 11mm) to the left.
Images:
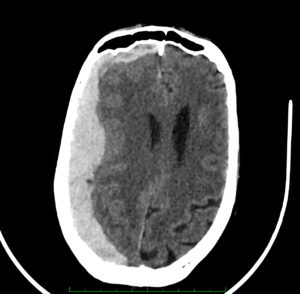
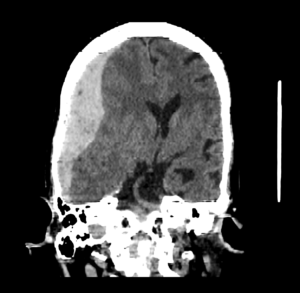

Conclusion: Subdural hemorrhage along the right tempero-fronto-parietal convexity causing mass effect and midline shift.
by Nithesh Ravindran | Sep 1, 2022
Sex: Male
Complaints: Left Flank pain.
Age: 48yr
Case study: Left kidney: 10.8 X 3.6 cm. Minimal perinephric free fluid with fat stranding noted. A calculus (~HU 581) measuring ~ 7.7 x 5.7 x 5.4 mm (CC x AP x TR)noted in the upper segment of left ureter with periureteric fat stranding through out its course.
Images:
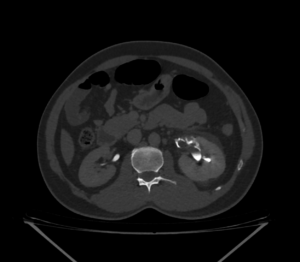




On contrast administration left kidney in delayed phase:
4 min delay image shows : No contrast transport in the ureter.
10 min delay image shows: No contrast transport in the ureter. There is evidence of contrast extravasation tracing from the renal hila extending circumferentially around proximal ureter confined to the upper segment.
20 min delay image shows: No contrast transport in the ureter. There is evidence of contrast extravasation tracing from the renal hila and mid calyx extending into the perinephric and periureteric region. There is irregular streaking of contrast extending into the adjacent perinephric plane both medially and laterally.
30 min delay images shows: No contrast transport in the left ureter. There is further more extravasation of contrast along the ureter caudally in addition to previously seen mentioned areas.
Conclusion: Left ureteric calculus with renal inflammatory changes in the form of perinephric fluid and fat stranding. Left kidney shows contrast leakage tracing from the hila as described in delayed phase with increase in area of spread proportionate to increase in time. – ?pelvic/calyceal rupture. Left ureter shows no contrast transport through out the multiple phase imaging study. No urinary bladder calculus.