by Nithesh Ravindran | Mar 15, 2023
Case courtesy : Dr.Cicy Kuncherian Welcare Hospital
Age: 56Yrs
Sex: Female
Complaints: Right iliac fossa pain.
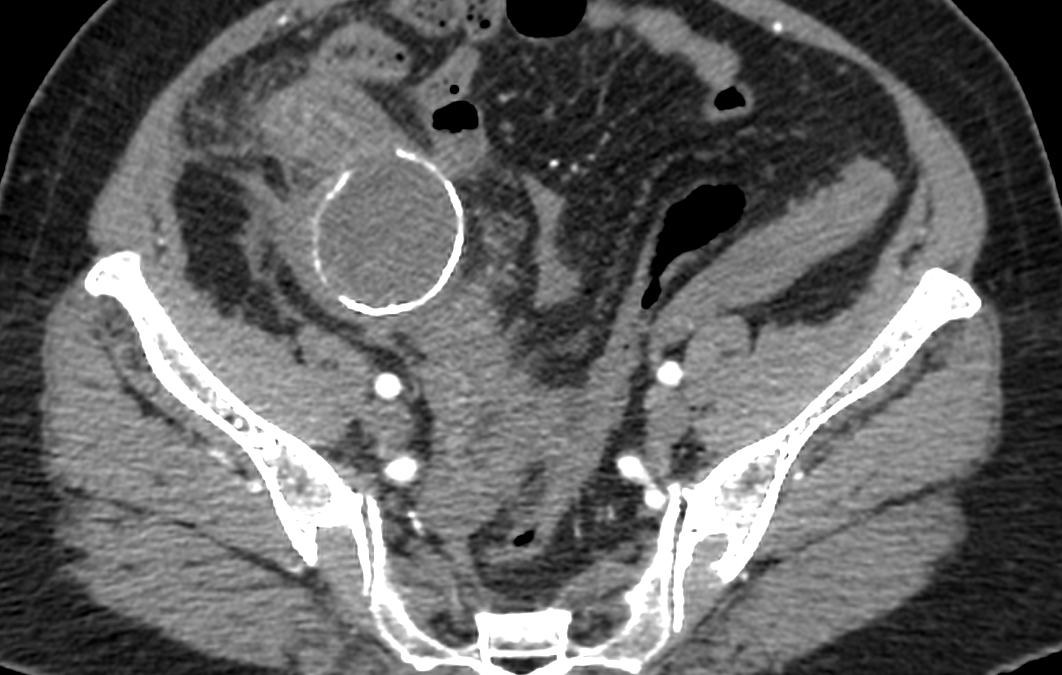
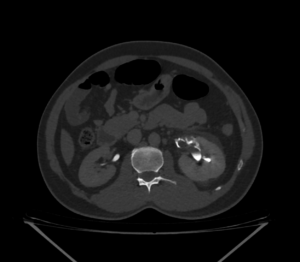
Case study: Tubular cystic mass lesion with peripheral enhancing walls measuring approximately 5.2 x4.3 x5.6 cm (TR XAP x CC) is seen in the right iliac fossa showing thick curvilinear mural calcification and central fluid density. No intraluminal air pockets noted.
The lesion is closely adherent towards the adjacent bowel loops causing bowel wall thickening of terminal ileum and cecum and adjacent fat stranding . Appendix not separately visualized from the mass lesion. Few prominent mesenteric lymph nodes are noted in right iliac fossa and paraumbilical region.
Small wall defect noted in the inferior aspect of the lesion with tubular extension measuring 14 x12mm extending into the right adnexa . Right ovary not separately
Images:



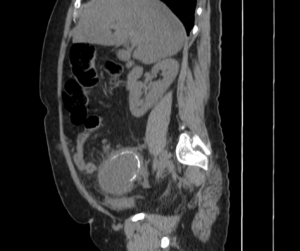

Conclusion : Tubular cystic mass lesion with curvilinear mural calcification in right iliac fossa with adjacent bowel wall thickening and fat stranding -features are in favor of Appendiceal Mucocele with contained perforation. Suggested lab correlation.
by Nithesh Ravindran | Sep 1, 2022
Sex: Male
Complaints: Left Flank pain.
Age: 48yr
Case study: Left kidney: 10.8 X 3.6 cm. Minimal perinephric free fluid with fat stranding noted. A calculus (~HU 581) measuring ~ 7.7 x 5.7 x 5.4 mm (CC x AP x TR)noted in the upper segment of left ureter with periureteric fat stranding through out its course.
Images:




On contrast administration left kidney in delayed phase:
4 min delay image shows : No contrast transport in the ureter.
10 min delay image shows: No contrast transport in the ureter. There is evidence of contrast extravasation tracing from the renal hila extending circumferentially around proximal ureter confined to the upper segment.
20 min delay image shows: No contrast transport in the ureter. There is evidence of contrast extravasation tracing from the renal hila and mid calyx extending into the perinephric and periureteric region. There is irregular streaking of contrast extending into the adjacent perinephric plane both medially and laterally.
30 min delay images shows: No contrast transport in the left ureter. There is further more extravasation of contrast along the ureter caudally in addition to previously seen mentioned areas.
Conclusion: Left ureteric calculus with renal inflammatory changes in the form of perinephric fluid and fat stranding. Left kidney shows contrast leakage tracing from the hila as described in delayed phase with increase in area of spread proportionate to increase in time. – ?pelvic/calyceal rupture. Left ureter shows no contrast transport through out the multiple phase imaging study. No urinary bladder calculus.
by Nithesh Ravindran | Jan 27, 2022
Name: Aneesh
Age: 28 Yrs
Sex: Male
Complaints:
Introduction:
Case study: A well-defined irregular non-enhancing hypodense cystic lesion measuring ~ 6.0 x 5.7 x 5.0 cm (CC x TR x AP) showing fluid attenuation (ranging +40 to -22HU) noted closely adjacent to the lower pole of right kidney and extending along the course of proximal ureter caudally for ~ 6.7 cm and significantly displacing it posteriorly.
The lesion is seen abutting the adjacent bowel loop superiorly and closely near to the psoas muscle posteriorly.
Images
Conclusion: Well-defined irregular non-enhancing hypodense cystic lesion in the right perirenal space and extending along the proximal ureter as described. – Features favor’s the possibility of Urinoma in the background of obstructive renal pathology. Suggested Aspiration cytology.
Reference :
by Nithesh Ravindran | Jan 20, 2022
Name: Rasheeda
Age: 33 Yrs
Sex: Female
Complaints: C/o bilateral pedal edema.
Introduction:
Case study: liver measures ~9.9 cm appears shrunken with coarsened echotexture and irregular margins. The portal vein appears normal (~8.4 mm). Free fluid noted in the perihepatic and subhepatic region.
Images
Conclusion: Liver appears shrunken with coarsened echotexture and irregular margins. There is evidence of ascites and splenomegaly as described. – Features are in favour of cirrhotic liver disease. Suggested LFT correlation.
Reference :
by Nithesh Ravindran | Dec 30, 2021
Name: Baiju
Age: 41 Yrs
Sex: Male
Complaints: Right hypochondrial pain.
Introduction: Case study: Right kidney shows duplex collecting system with non functioning lower pole moiety showing ballooning of calyces in the mid and lower pole. There is no evidence of contrast excretion/draining noted in the obstructed collecting system arising from the mid and lower pole moiety.
The upper moiety of right kidney shows separate collecting system with normal excretion of contrast and no evidence of contrast delay.
The lower moiety is non traceable beyond the proximal aspect.
Left kidney shows normal concentration and excretion of contrast media.
Bilateral perinephric fat and para renal fascias are normal. Renal vessels are normal in caliber, course and opacification.
Images
Conclusion: Duplex collecting system with non functioning lower moiety of right kidney with obstructive hydronephrosis as described.
No evidence of ureterocele seen in the present study.
Reference :
by Nithesh Ravindran | Dec 30, 2021
Name: Unnikrishnan Pillai
Age: 60 Yrs
Sex: Male
Complaints: RIF tenderness.
Introduction: RIF: Probe tenderness present. Appendix not visualized. No evidence of free fluid.
Multiple enlarged right iliac lymphnodes noted, largest measuring ~13 x 6 mm with fatty hilum and oval shape.
A well defined heteroechoic solid appearing mass measuring ~4.6 x 2.1 cm noted in the right iliac region. Minimal surrounding vascularity noted.
Case study:
Images
Conclusion: A well defined heterogenous mass in the right iliac fossa with moderate probe tenderness and enlarged mesenteric lymphnodes. – Features suggestive of appendicular mass.
Suggested CT Abdomen for further evaluation.
Reference :